Introduction
According to the CDC, U.S. acute-care hospitals recorded an estimated 687,000 healthcare-associated infections (HAIs) in 2015, with approximately 72,000 patient deaths among hospitalized patients with HAIs. The direct medical cost to hospitals runs between $28.4 billion and $45 billion annually, depending on the inflation adjustment method used.
Those numbers translate directly to operational strain. A 2021 prospective study found HAIs add an average of 7.8 excess hospital days per affected patient. In cardiac surgery specifically, a major HAI was linked to nearly $38,000 in incremental cost, 14 additional inpatient days, and 8.7% of all readmissions.
The bulk of that burden is preventable. Standard precautions — applied by every clinician, on every patient encounter — are the primary tool for stopping transmission before it starts.
This guide covers what standard precautions are and their core components, how transmission-based precautions layer on top, and the most common compliance failures that put patients and staff at risk.
Key Takeaways
- Standard precautions apply to every patient, every encounter, every setting — regardless of known infection status
- Core components include hand hygiene, PPE, respiratory hygiene, safe injection practices, and environmental cleaning
- Transmission-based precautions (contact, droplet, airborne) layer on top of standard precautions, not in place of them
- Patient placement is a formal infection control component, not an afterthought
- Non-adherence remains the biggest failure point — studies show fewer than 28% of nurses and nursing assistants follow contact precaution protocols correctly
What Are Standard Precautions for Infection Control?
Standard precautions are the minimum set of infection prevention and control practices that all healthcare workers must apply to every patient encounter, in every care setting, regardless of whether a patient is known or suspected to be infectious.
The CDC defines them as practices based on risk assessment that use common-sense work habits and appropriate PPE to protect both healthcare personnel and patients. The WHO's 2022 aide-memoire reinforces this: standard precautions apply to all patients, at all times, in all settings, targeting both recognized and unrecognized infection sources.
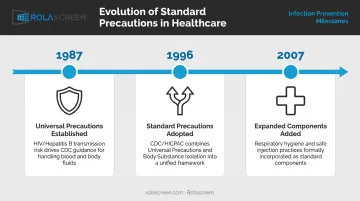
From Universal Precautions to the Two-Tier Framework
The concept evolved over several decades:
- 1987: CDC's MMWR recommended treating blood and certain body fluids from all patients as potentially infectious for HIV and hepatitis B — establishing Universal Precautions
- 1996: CDC/HICPAC merged Universal Precautions with Body Substance Isolation into the broader Standard Precautions framework, extending coverage to all body fluids (except sweat), non-intact skin, and mucous membranes
- 2007: CDC/HICPAC added respiratory hygiene/cough etiquette and safe injection practices as formal components
The Two-Tier Structure
| Tier | Name | Applies To |
|---|---|---|
| Tier 1 | Standard Precautions | Every patient, every encounter |
| Tier 2 | Transmission-Based Precautions | Patients with known or suspected transmissible pathogens |
Tier 2 is always layered on top of Tier 1 — never substituted for it.
Two separate bodies govern compliance with these tiers:
- OSHA (29 CFR 1910.1030) sets the enforceable worker-protection floor for occupational exposure to blood and other potentially infectious materials (OPIM)
- CDC/HICPAC provides the clinical infection control framework that guides practice at the bedside
- Non-compliance carries legal, accreditation, and patient safety consequences
The Core Components of Standard Precautions
Standard precautions function as an interconnected system. Skipping any one component undermines the protective effect of the others. There are ten recognized elements — the highest-yield components are covered in detail below.
Hand Hygiene
Hand hygiene is the single most effective infection prevention measure, yet it remains one of the most inconsistently performed.
When hand hygiene is required (WHO's Five Moments):
- Before touching a patient
- Before a clean or aseptic procedure
- After body fluid exposure
- After touching a patient
- After touching patient surroundings
Missed hand hygiene opportunities among healthcare personnel can reach 50%, according to CDC STRIVE. An observational study reported compliance rates as low as 20.3% across some measured moments.

Which method to use:
- Alcohol-based hand rub (ABHR): Preferred in most clinical situations: faster, more accessible, and clinically effective
- Soap and water: Required when hands are visibly soiled, after using the restroom, and during C. difficile outbreaks (physically removes spores that ABHR cannot kill)
Personal Protective Equipment (PPE)
PPE selection under standard precautions is risk-based, not uniform. The right PPE depends on the anticipated exposure.
| PPE Type | Required When |
|---|---|
| Gloves | Contact with blood, body fluids, mucous membranes, non-intact skin, or contaminated items |
| Gown | Splash/spray risk present, or contact with heavily contaminated environments |
| Surgical mask | Splash to face possible; source control for symptomatic individuals |
| N95 respirator | Aerosol-generating procedures with suspected respiratory pathogens |
| Eye protection | Splash or spray to eyes or face is possible |
Donning sequence (CDC): Gown → mask/respirator → goggles/face shield → gloves
Doffing sequence (CDC): Gloves → goggles/face shield → gown → mask/respirator (mask removed after leaving and closing the patient-room door)
Doffing carries the highest contamination risk. A 2015 JAMA Internal Medicine study found 46% of PPE removal simulations resulted in skin or clothing contamination, with glove removal being the highest-risk step at 52.9%. Perform hand hygiene immediately if contamination occurs during removal.
Respiratory Hygiene and Cough Etiquette
Respiratory hygiene targets patients, visitors, and staff alike. It functions as a source control strategy, reducing the volume of respiratory particles released into shared air.
Core practices:
- Cover coughs and sneezes with a tissue or inner elbow
- Dispose of tissues immediately; do not set them down on surfaces
- Perform hand hygiene after any respiratory contact
- Mask symptomatic individuals at facility entrances and in waiting areas
Facilities must keep supplies — masks, hand sanitizer dispensers, tissues, and no-touch waste receptacles — available at entry points, triage areas, and waiting rooms, not just at care stations.
Safe Injection and Sharps Practices
Approximately 385,000 sharps injuries occur annually among hospital-based healthcare personnel. OSHA estimates that 62–88% of those injuries are preventable with safer medical devices and proper technique.
Core rules:
- Never recap, bend, or break contaminated needles
- Use a single-use needle and syringe per injection — never reuse
- Dispose of sharps immediately into a puncture-proof, labeled sharps container
- Select safety-engineered devices through an annually reviewed exposure-control plan that includes input from frontline staff
The primary risks are bloodborne pathogens: HIV, Hepatitis B, and Hepatitis C. OSHA's standard requires treating sharps safety as a device-selection issue, not just a technique issue.
Environmental Cleaning and Waste Management
All patient care equipment soiled with blood, body fluids, or excretions must be handled to prevent skin/mucous membrane exposure, clothing contamination, and transfer to other patients.
- Single-use items: Discard after use
- Reusable items: Clean and reprocess before the next patient contact
- Disinfectants: Must be EPA-registered and matched to the target organism (EPA maintains specific lists for C. difficile, MRSA/VRE, Candida auris, and SARS-CoV-2)
Regulated vs. non-regulated waste under OSHA 29 CFR 1910.1030:
Regulated medical waste includes:
- Liquid or semi-liquid blood or other potentially infectious materials (OPIM)
- Items caked with dried blood capable of releasing material during handling
- Contaminated sharps
- Pathological or microbiological wastes
General clinical trash that does not meet these criteria is not regulated waste. The distinction must be made deliberately, not assumed.
Transmission-Based Precautions: The Second Tier
Transmission-based precautions are added when a patient is known or suspected to carry a pathogen requiring additional containment. They escalate the PPE and environmental requirements — but standard precautions remain in full effect throughout.
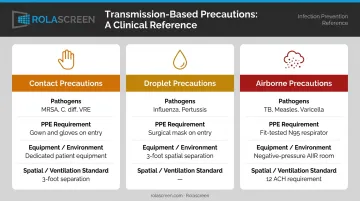
The Three Categories
Contact Precautions — for pathogens spread by direct or indirect touch (MRSA, C. difficile, VRE, norovirus):
- Gown and gloves on room entry
- Single-patient room preferred; if unavailable, minimum 3-foot separation with privacy curtains
- Dedicated or disposable patient care equipment (BP cuffs, stethoscopes)
Droplet Precautions — for pathogens spread via respiratory droplets at close range (influenza, pertussis, adenovirus):
- Surgical mask on room entry
- Single-patient room preferred; spatial separation of at least 3 feet when cohorting
Airborne Precautions — for pathogens that remain suspended in air over long distances (tuberculosis, measles, varicella):
- Fit-tested NIOSH-approved N95 or higher respirator before entry
- Airborne Infection Isolation Room (AIIR) with monitored negative pressure
- 12 air changes per hour (ACH) for new construction; 6 ACH minimum for existing facilities
- Exhaust directed outside or through HEPA filtration
Isolation and Patient Outcomes
Isolation precautions are necessary — but they carry measurable secondary risks when not actively managed. Published clinical research has documented that patients under isolation precautions experience 31 adverse events per 1,000 days compared to 15 for non-isolated patients, along with longer lengths of stay and less frequent clinical contact. Isolation must not reduce the frequency or quality of patient assessment — rounding schedules and nursing check-ins should remain unchanged regardless of precaution tier.
Patient Placement and Environmental Controls
Appropriate patient placement is a formal component of standard precautions. Where a patient is located directly affects transmission risk.
Placement priorities (CDC guidance):
- Single-occupancy rooms are preferred for contact and droplet precautions when available
- When rooms are limited, prioritize single rooms for patients with uncontained drainage, stool incontinence, excessive cough, or conditions that amplify transmission
- Cohort patients with the same confirmed pathogen when single rooms are unavailable
- Patients requiring airborne precautions must be placed in an AIIR or transferred if none is available
High-Touch Surface Management
Environmental surfaces are a documented vector for pathogen transfer. Research from Li et al. (2025) found HAI incidence positively correlated with high-touch surface contamination levels — with infection risk increasing approximately 23% for each IQR increase in total colony count.
Surfaces requiring consistent attention:
- Bed rails, call buttons, door handles
- IV poles, infusion pump controls
- Privacy curtain hardware
All must be cleaned with EPA-registered disinfectants appropriate to the organisms present. "Visually clean" is not the same as disinfected.
Physical Separation in Open-Bay Environments
In emergency departments, open-bay treatment areas, and multi-station clinical spaces, single rooms are frequently unavailable. In these settings, retractable physical barriers can separate patients effectively — but the panel material determines whether they actually support infection control compliance.
Rolascreen's medical privacy screens are deployed in EDs, isolation units, and infusion bays at facilities including Kaiser Permanente, UCSF, and VA hospitals. Their non-porous polyester film panels are compatible with the full range of disinfectants used in contact precaution protocols:
- Bleach solutions up to 10,000 ppm (above the CDC's 5,000 ppm sporicidal threshold for C. difficile)
- Quaternary ammonium compounds
- Accelerated hydrogen peroxide disinfectants
Unlike fabric privacy curtains, which cannot be reliably disinfected between patients, these panels wipe down between every patient encounter — no room modification required.
Common Standard Precaution Mistakes That Increase Infection Risk
Most HAIs are not caused by a single catastrophic failure. They result from repeated small compliance gaps across routine clinical workflows.
Treating Gloves as a Substitute for Hand Hygiene
Gloves reduce pathogen transfer during patient contact, but they do not eliminate it. The critical moment is after removal: contaminated gloves transfer pathogens to clean surfaces during doffing, and many clinicians skip hand hygiene at that step.
A 2021 observational study found hand disinfection occurred before glove use in only 18.6% of cases and after glove removal in 65.1%. That means roughly one in three post-glove encounters involved no hand hygiene at all.
Incorrect PPE Donning and Doffing Sequence
A 2019 study published in the Journal of Occupational and Environmental Hygiene observed 162 doffing events — 90% were incorrect in sequence, technique, or PPE selection. Putting on a gown after entering a contaminated environment, or removing gloves before the gown, defeats containment entirely.
Sustained compliance requires posted visual guides at the point of care, regular competency checks, and direct observation with real-time feedback — not just onboarding training.
Assuming Shared Equipment Is Clean Enough
Equipment contamination is another gap that onboarding checklists rarely close. "Visually clean" is a judgment call, not an infection control standard.
- Non-disposable BP cuffs showed 70% contamination before decontamination in a controlled study
- A review of 28 stethoscope studies found a mean contamination rate of 85%

Shared noncritical equipment — BP cuffs, stethoscopes, thermometers, IV poles — must be dedicated to a single patient or disinfected between every patient contact. The disinfectant must also match the pathogen present; a product effective against MRSA may not be sporicidal for C. difficile.
Conclusion
Standard precautions are not triggered by visible illness or a positive test result. They operate under the assumption that any patient encounter carries potential transmission risk — which means every component, applied to every patient, every time.
That universal scope is also where compliance breaks down. A clinician who performs hand hygiene consistently but skips post-doffing hygiene, or a facility that stocks appropriate PPE but doesn't enforce doffing sequence, offers no meaningful safety advantage over a facility with no protocol at all. Partial adherence creates predictable gaps — and predictable gaps produce preventable infections.
Sustained low HAI rates come from treating standard precautions as an operational commitment, not a documentation exercise. That means:
- Monitoring adherence through direct observation and audit cycles
- Educating staff on doffing sequence, hand hygiene timing, and equipment selection
- Provisioning appropriate PPE at the point of care, not just in supply rooms
- Designing physical environments that reduce cross-contamination opportunities
Facilities that do this consistently don't just have better policies — they have measurably better outcomes.
Frequently Asked Questions
What are the standard precautions for infection control?
Standard precautions are the minimum infection prevention practices applied to all patient care, in all settings, regardless of known infection status. They cover hand hygiene, PPE use, respiratory hygiene, safe injection practices, environmental cleaning, and appropriate patient placement, as defined by the CDC and WHO.
What is the difference between standard precautions and transmission-based precautions?
Standard precautions are the universal Tier 1 baseline applied to every patient. Transmission-based precautions (contact, droplet, and airborne) are Tier 2 additions layered on top when a specific infectious pathogen requires extra containment. Standard precautions remain in effect throughout.
Who is required to follow standard precautions?
All healthcare workers are required to follow standard precautions: physicians, nurses, nursing assistants, technicians, housekeeping staff, and anyone entering a patient care environment. Visitors are subject to facility-specific policies that typically mirror the same principles.
What PPE is required under standard precautions?
PPE selection is risk-based, not uniform. Gloves are required for contact with blood and body fluids; gowns when splash risk exists; surgical masks and eye protection when airborne or splash exposure to the face is possible. The anticipated exposure determines what is needed for each encounter.
When should soap and water be used instead of hand sanitizer?
Soap and water is required when hands are visibly soiled, after using the restroom, and during C. difficile outbreaks because physical washing removes spores that alcohol-based hand rub cannot neutralize. In all other routine clinical situations, alcohol-based hand rub is the CDC-preferred method.
What infections require transmission-based precautions on top of standard precautions?
Contact precautions are added for MRSA, C. difficile, and VRE; droplet precautions for influenza and pertussis; airborne precautions for tuberculosis, measles, and varicella. The CDC's Appendix A provides a comprehensive list of infections with required precaution type and duration.