The problem isn't just inadequate cleaning — it's what happens between cleaning cycles. Research shows bacterial counts on bed rails and overbed tables rebound from 3.46 CFU/cm² at 4 hours to 5.27 CFU/cm² at 48 hours after cleaning. Standard disinfectants leave no residual activity, meaning surfaces are re-contaminated almost immediately.
Antimicrobial surfaces address this gap. They don't replace cleaning — they reduce the microbial burden between cleaning intervals, creating a layered defense that standard protocols alone can't achieve.
This article covers what antimicrobial surfaces are, which hospital surfaces pose the highest risk, what technologies actually work, and how to select and implement them effectively.
Key Takeaways
- 1 in 31 hospital patients acquires an HAI; bacterial surface contamination rebounds within hours of cleaning
- High-touch surfaces — bed rails, IV poles, keyboards, stretcher rails — carry the greatest transmission risk
- Copper-alloy surfaces have the strongest clinical evidence, cutting HAI rates from 0.081 to 0.034 per patient-day
- Fabric curtains contaminate within one week; non-porous wipeable alternatives eliminate this harborage point
- Antimicrobial surfaces work best as part of a layered strategy alongside hand hygiene and cleaning protocols
What Are Antimicrobial Surfaces?
Antimicrobial surfaces fall into two categories:
- Passive antimicrobial surfaces — non-porous, smooth materials that resist bacterial attachment and biofilm formation by design, making them easier to disinfect completely
- Active antimicrobial surfaces — materials or coatings that continuously destroy pathogens through biocidal mechanisms (copper ions, silver compounds, organosilane agents)
Why Standard Cleaning Isn't Enough
Disinfectants work on contact, but that protection stops the moment the surface dries. The Bogusz et al. study tracking 360 sites across 30 hospital bed spaces found that aerobic colony counts dropped immediately after cleaning, then steadily climbed over the next 48 hours. By day two, contamination had nearly returned to pre-cleaning levels — during the very window when rooms aren't being actively cleaned, which is most of the time. Antimicrobial surfaces reduce that baseline microbial load precisely in this gap.
Regulatory Context
The Joint Commission's infection prevention standards require facilities to maintain documented procedures for cleaning and disinfecting patient care spaces, surfaces, and equipment. While neither the Joint Commission nor WHO has issued explicit directives mandating antimicrobial surfaces specifically, WHO's 2022 global IPC report notes that comprehensive IPC programs can reduce healthcare infections by 70% — and surface selection has become part of that equation.
In practice, this means facilities face two distinct obligations:
- Required: Documented cleaning and disinfection procedures for all patient care surfaces
- Emerging standard: Material selection that supports IPC goals, including non-porous, wipeable surfaces
High-Touch Hospital Surfaces: The Hidden HAI Threat
Not all hospital surfaces carry equal risk. The surfaces touched most frequently by patients, staff, and visitors create the most direct pathogen transmission pathways.
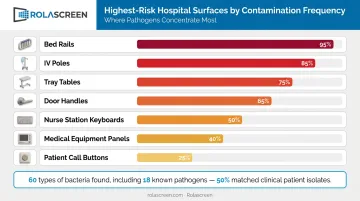
The Highest-Risk Surfaces
The CDC identifies these as priority high-touch surfaces in patient care areas:
- Bed rails and bed frames
- IV poles and blood pressure cuffs
- Tray tables and bedside tables
- Door handles and light switches
- Nurse station keyboards
- Medical equipment control panels
- Patient call buttons
A 2024 study at the Central Texas Veterans Healthcare System sampled 400 surfaces — including bed rails, workstations on wheels, and nurse station keyboards — and identified 60 types of bacteria, including 18 known human pathogens. MRSA, VRE, E. coli, and Pseudomonas aeruginosa were among those found, and approximately 50% of bacteria on surfaces matched clinical isolates from patients during the same period.
The Portable Equipment Problem
Mobile equipment — patient transport stretchers, workstations on wheels, portable monitors — presents a unique challenge. These items move between rooms and departments, potentially carrying contamination across an entire floor in a single shift. Room-based disinfection strategies can't address cross-departmental spread through mobile equipment, which is why stretcher rails and portable workstations appear repeatedly in HAI-related research.
Textiles and Privacy Curtains: An Overlooked Reservoir
Unlike mobile equipment, privacy curtains stay in place — yet they're among the most consistently contaminated surfaces in hospital rooms and often the last to receive attention.
A longitudinal study by Ohl et al. tracking 43 curtains found:
- 95% were contaminated at least once
- 92% of brand-new curtains became contaminated within one week of installation
- MRSA was present on 21% of curtains; VRE on 42%
Standard disinfectant wipes can't penetrate fabric fibers — the only options are replacement or laundering, neither of which happens frequently enough.
Non-porous, wipeable alternatives address this directly. Rolascreen's retractable privacy screens use smooth polyester film panels compatible with EPA-registered hospital disinfectants, including bleach at concentrations up to 10,000 ppm — well above the CDC's 5,000 ppm sporicidal threshold for C. difficile. The panels wipe down between patients using the same protocols already applied to bed rails and IV poles.
Types of Antimicrobial Surface Technologies in Healthcare
Metal-Based Antimicrobial Surfaces
Copper is the most clinically validated antimicrobial surface material in healthcare. Copper ions continuously disrupt bacterial cell membranes and destroy pathogens on contact, including between cleaning cycles.
The strongest clinical evidence comes from Salgado et al.'s randomized ICU trial, which found:
- HAI rate: 0.034 in copper rooms vs. 0.081 in standard rooms (P = .013)
- HAI and/or MRSA/VRE colonization: 0.071 vs. 0.123 (P = .020)
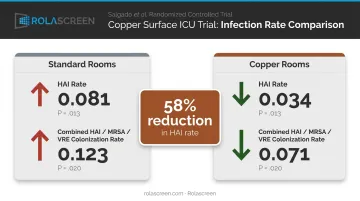
That's a meaningful, statistically significant reduction in patient outcomes — not just surface contamination counts. Silver-based surfaces have also shown antimicrobial properties, though the clinical outcome evidence is less extensive than for copper.
The limitation: copper alloy surfaces require replacing existing equipment components, which is capital-intensive. Implementation is most practical for select high-touch items (bed rails, door handles, IV poles) rather than facility-wide retrofitting.
Antimicrobial Surface Coatings
Given the capital cost of copper replacement, coatings offer a more accessible path: applying biocidal activity to existing surfaces without swapping out components. Technologies include modified acrylate-silane compounds, organosilane agents, and nanoparticle-based formulations.
The ASEPTIC pilot RCT tested NOMOBAC (a modified acrylate-silane coating) on 96 stretcher rails in a Singapore emergency department. At 24 hours:
- Total aerobic bacteria: 0.61 CFU/cm² (coated) vs. 1.01 CFU/cm² (placebo)
- Rails exceeding 2.50 CFU/cm²: 14.6% (coated) vs. 22.9% (placebo)
Useful data, though the study was a single-center pilot with no patient-outcome endpoint. Durability is the primary limitation across this category: repeated wiping and adhesive stripping degrade performance over time, and organosilane coatings have shown mixed results under real-world patient room conditions.
Non-Porous and Inherently Cleanable Surfaces
Surface material selection during hospital design and equipment procurement is often underestimated. Rougher surfaces — ceramic tile grout, brushed stainless steel, textured polymers — provide more surface area for bacterial attachment and biofilm scaffolding. Smooth, non-porous materials resist initial adhesion and allow complete disinfection with each wipe.
Key material characteristics to evaluate during procurement:
- Surface texture: Non-porous, smooth finishes resist biofilm formation; avoid brushed steel or textured polymers in high-touch zones
- Disinfectant compatibility: Verify approved cleaning agents before purchase
- Wipe durability: Material must withstand repeated EPA-registered disinfectant application without surface degradation
Disinfectant compatibility deserves particular attention. The Philips Respironics ventilator and CPAP recall (June 2021) illustrates what happens when it's overlooked: PE-PUR sound abatement foam degraded when exposed to ozone and UV cleaning methods not approved for those devices, potentially exposing patients to chemical particles.
Microscopic surface damage from incompatible disinfectants creates the same problem at smaller scale — harborage points where pathogens accumulate between cleanings.
Key Benefits of Antimicrobial Surfaces for Patient Safety
Clinical Impact
A 2020 systematic review in the Journal of Hospital Infection (Albarqouni et al.) found low-quality evidence that copper-treated commonly touched surfaces reduced HAIs by 27%. The copper ICU trial by Salgado et al. provides the clearest patient-outcome signal — significant reductions in both HAI rates and MRSA/VRE colonization.
Financial Impact
HAIs carry substantial costs. Research published in JAMA Internal Medicine estimated per-case costs:
| Infection Type | Estimated Cost Per Case |
|---|---|
| Central line-associated bloodstream infection (CLABSI) | $45,814 |
| Ventilator-associated pneumonia (VAP) | $40,144 |
| Surgical site infection (SSI) | $20,785 |
| C. difficile infection | $11,285 |
| Catheter-associated UTI (CAUTI) | $896 |
Total annual cost across these five HAI types was estimated at $9.8 billion in U.S. hospitals. Beyond direct treatment costs, CMS's Hospital-Acquired Condition Reduction Program applies a 1% payment reduction to hospitals in the worst-performing quartile on HAI measures — creating direct financial accountability for infection rates.
Operational and Staff Benefits
- Reduced HAI rates mean shorter patient stays and lower liability exposure
- Healthcare workers are exposed to the same contaminated surfaces as patients — antimicrobial surfaces protect staff as well
- In high-turnover areas like emergency departments, cleaning between every patient encounter isn't always feasible — surfaces with lower baseline contamination reduce transmission risk when cleaning frequency falls short
Best Practices for Selecting and Implementing Antimicrobial Surfaces
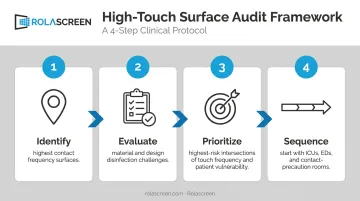
Start With a High-Touch Surface Audit
Before procurement, map your facility:
- Identify which surfaces in each care area have the highest contact frequency
- Evaluate which are currently difficult to disinfect due to material or design (textured surfaces, fabric, complex geometry)
- Prioritize antimicrobial surface solutions for the highest-risk intersections of touch frequency and patient vulnerability
- Sequence implementation — start with ICUs, EDs, and contact-precaution rooms before lower-acuity areas
A facility-wide overhaul attempted simultaneously rarely succeeds. Targeted, evidence-aligned deployment delivers better outcomes and clearer ROI.
Apply a Compatibility-First Framework
Before any antimicrobial surface or coating is purchased, confirm:
- Verify compatibility with every disinfectant category used in your facility: quaternary ammonium compounds, bleach-based, accelerated hydrogen peroxide, alcohol-based, and peracetic acid
- Confirm manufacturer IFUs align with your infection prevention protocols (contact times, concentrations, application methods)
- Review wear testing for the specific use environment — adhesive wear for stretcher rail coatings, repeated wiping for privacy partitions, mechanical stress for bed rail components
This is especially critical for coated surfaces. A coating that performs well at 30 days but degrades by 90 days provides false assurance if re-application schedules aren't built into procurement planning.
Integrate Into a Layered Strategy
Antimicrobial surfaces are not a substitute for hand hygiene compliance, cleaning schedules, or staff training. They're a complement. The most effective infection control programs combine:
- Maintain hand hygiene compliance as the foundation of any infection control program
- Clean consistently with EPA-registered disinfectants as the primary environmental intervention
- Deploy antimicrobial surfaces to reduce microbial burden between cleaning intervals
- Establish monitoring and re-evaluation protocols to confirm surface investments are delivering measurable reductions in contamination and HAI rates
Privacy barriers are one area where the layered approach is easy to overlook. Fabric curtains are notoriously difficult to disinfect and are a well-documented textile-based contamination source.
Rolascreen's retractable privacy screens replace fabric curtains with smooth, non-porous panels compatible with standard EPA-registered disinfectants. Deployed at Kaiser Permanente, UCSF, UCLA, and VA hospitals, they fit into existing cleaning workflows without construction or permanent installation.
Frequently Asked Questions
What are antimicrobial surfaces?
Antimicrobial surfaces are materials or coatings engineered to inhibit microbial growth — either passively (non-porous surfaces that resist bacterial attachment) or actively (copper ions, silver compounds, or biocidal coatings that destroy pathogens on contact). In hospitals, they supplement routine cleaning rather than replace it.
Do hospitals use antimicrobial sheets?
Some hospitals use antimicrobial-treated linens, but standard sheets typically are not. Higher-impact investments target hard surfaces and equipment — replacing porous textiles like privacy curtains with non-porous, wipeable alternatives that can be fully disinfected between patients.
What are the top 5 chemical disinfectants used in hospitals?
The most common EPA-registered categories are: quaternary ammonium compounds, sodium hypochlorite (bleach), accelerated hydrogen peroxide, isopropyl or ethyl alcohol, and peracetic acid.
What surfaces in hospitals are considered high-touch areas?
The most frequently contaminated surfaces include bed rails, patient call buttons, door handles, IV poles, nurse station keyboards, stretcher rails, medical equipment control panels, and privacy curtains or partitions.
How do antimicrobial surfaces help reduce healthcare-associated infections?
Standard disinfection has no residual activity — contamination rebounds within hours of cleaning. Antimicrobial surfaces reduce the microbial burden during those intervals. This lowers the probability that a pathogen transfers from a surface to a patient or healthcare worker before the next cleaning cycle.