The stakes are high. CDC estimates that 1 to 3 million serious infections occur in long-term care settings every year, and residents face far greater vulnerability than the general population due to age, chronic illness, and shared living quarters.
This guide covers why LTCFs are high-risk environments, the infections most commonly reported, the five core IPC principles, standard and transmission-based precautions, resident placement strategies, and outbreak preparedness — including what CMS now requires under the 2024 Enhanced Barrier Precautions update.
Key Takeaways
- UTIs, respiratory infections, and skin/soft tissue infections are the most prevalent LTCF infection types
- More than 50% of nursing home residents may be colonized with a multidrug-resistant organism (MDRO)
- Federal regulations (CMS 42 CFR 483.80) require a formal IPC program, a designated infection preventionist, and antibiotic stewardship
- Enhanced Barrier Precautions (April 2024) mandate gown and gloves during high-contact care for residents with chronic wounds or indwelling devices
- Most LTCFs rely on private rooms and cohorting for isolation — purpose-built infrastructure remains rare
Why Long-Term Care Facilities Are High-Risk Infection Environments
Resident Risk Factors
LTCF residents carry multiple overlapping vulnerabilities that compound infection risk:
- Immunosenescence — age-related immune decline that reduces the ability to fight off pathogens
- Chronic conditions — diabetes, COPD, heart failure, and dementia each impair normal immune defense
- Indwelling devices — urinary catheters, feeding tubes, and central lines create direct pathogen entry points
- Chronic wounds — pressure injuries and surgical wounds that don't fully heal
- Shared living spaces — communal dining, shared bathrooms, and multi-bed rooms increase exposure density

Each factor amplifies the others. Combined, they make LTCFs one of the most challenging infection control environments in healthcare.
The Regulatory Landscape
CMS addressed this risk in 2016 when it published a final rule under 42 CFR 483.80, requiring every LTCF to maintain a formal infection prevention and control program (IPCP), designate a qualified infection preventionist with at least part-time hours and specialized training, and operate an antibiotic stewardship program.
Compliance has been uneven. Research published in the Journal of the American Medical Directors Association found that 57% of freestanding nursing homes received at least one F880 Infection Prevention and Control deficiency citation between November 2017 and November 2019 — and 15% were cited more than once.
Balancing Infection Control With Resident Rights
CMS guidelines make clear that infection control cannot come at the cost of resident autonomy. Residents retain the right to participate in group activities, receive visitors, and move freely within the facility. The 2024 Enhanced Barrier Precautions guidance specifically states that residents under EBP are not restricted to their rooms and are not barred from group activities. For IPC coordinators, this means infection control must be built into routine care practices — not enforced through movement restrictions.
Most Common Infections in Long-Term Care Settings
Endemic Infections
Nursing home infection surveillance consistently identifies three dominant categories:
- Urinary tract infections (UTIs) — most frequently reported in LTCFs, though symptomatic UTI rates vary depending on the diagnostic criteria applied
- Respiratory infections — pneumonia and influenza are leading causes of hospitalization and mortality
- Skin and soft tissue infections — wound infections, cellulitis, and infected pressure injuries
A 2023 Pennsylvania LTC surveillance report analyzing nearly 24,000 infection reports found respiratory tract infections accounted for 34.3% of reported cases, UTIs 25.5%, and skin/soft tissue infections 17.9%.
The MDRO Problem
Beyond endemic infections, multidrug-resistant organisms — MRSA, C. difficile, CRE, VRE — present a separate and harder-to-detect challenge. Colonized residents show no symptoms: no fever, no wound, no clinical indicator that anything is wrong.
Research across 28 nursing homes found a median MDRO colonization prevalence of 50% among residents, with individual facility rates ranging from 24% to 70%. More than half of nursing homes had more than half of their residents colonized.
The hospital-to-LTCF transfer cycle amplifies this further. Modeling research in JAMA Network Open shows that MDROs spread through regional healthcare networks as patients move between acute and post-acute settings. A resistant organism introduced by one newly admitted resident can reach the broader facility population within days.
The 5 Core Principles of Infection Prevention and Control
Principle 1 — Surveillance and Detection
Active surveillance is the foundation that everything else builds on. Facilities must track infection rates, monitor lab results for resistant organisms, and report communicable diseases to public health authorities.
A 2025 AJIC Florida needs assessment found that 53.4% of skilled nursing facilities reported having a formal surveillance plan — compared to just 8.4% of assisted living facilities. Without consistent surveillance, outbreaks go undetected until they're already established.
Principle 2 — Standard and Transmission-Based Precautions
Standard precautions apply to every resident, every encounter, regardless of known infection status. They include hand hygiene, PPE based on anticipated exposure, respiratory hygiene, and safe injection practices.
Transmission-based precautions layer on top when a specific pathogen is identified:
| Precaution Type | Pathogen Examples | Key Requirements |
|---|---|---|
| Contact | MRSA, C. diff, CRE | Gown + gloves on room entry |
| Droplet | Influenza, RSV | Surgical mask within 3 feet |
| Airborne | TB, measles, varicella | N95 + negative pressure room |
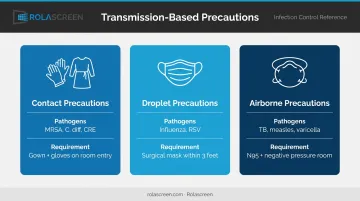
Both tiers operate simultaneously. Starting transmission-based precautions does not replace or reduce standard precaution requirements.
Principle 3 — Hand Hygiene
Hand hygiene is the single most effective intervention for breaking the chain of infection. The WHO Five Moments for Hand Hygiene define five critical points: before patient contact, before an aseptic task, after body fluid exposure risk, after patient contact, and after contact with the patient's surroundings.
Alcohol-based hand rub (60–95% alcohol) covers most clinical encounters. Soap and water is required in three situations:
- Hands are visibly soiled
- After contact with bodily fluids
- Following care for residents with C. difficile
Compliance rates in LTCFs remain a persistent problem. A 2022 observational study found mean hand hygiene compliance of just 14.7% across LTCF settings, with facility-level rates ranging from 1.4% to 29.1%.
Principle 4 — Environmental Cleaning and Disinfection
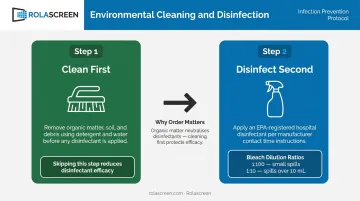
Cleaning and disinfection are two distinct steps, and order matters:
- Clean first — remove organic matter with detergent and water
- Disinfect second — apply EPA-registered hospital disinfectant to decontaminated surfaces
Skipping step one reduces disinfectant efficacy. For bodily fluid spills, CDC guidance specifies a 1:100 bleach dilution for routine small spills; for larger spills (>10 mL), begin with a 1:10 dilution to address heavy contamination before terminal disinfection.
High-touch surfaces — doorknobs, bedrails, call buttons, faucet handles — require daily attention. Laundry and bedding should be washed at a minimum of 160°F (71°C) for 25 minutes, handled with minimal agitation, and transported in sealed bags.
Principle 5 — Antibiotic Stewardship
CMS requires LTCFs to maintain antibiotic stewardship programs under 42 CFR 483.80, including written antibiotic-use protocols and a system to monitor antibiotic use. Antibiotics should be prescribed only when clinically indicated — reducing the selective pressure that drives resistance.
This matters especially in LTCFs, where residents frequently transfer between acute and post-acute settings and where inconsistent prescribing directly fuels MDRO colonization rates.
Standard Precautions: PPE, Environmental Cleaning, and Immunization
Appropriate PPE Use
LTCF staff should have access to and training on the full spectrum of required PPE:
- Gloves — required for contact with blood, bodily fluids, mucous membranes, or non-intact skin
- Isolation gowns — required for contact precautions; also for Enhanced Barrier Precautions
- Surgical masks — required when entering a droplet precaution room
- N95 respirators — required for airborne precautions; must be fit-tested
- Eye protection — goggles or face shields when splash or spray is anticipated
Enhanced Barrier Precautions (EBP) are a 2024 regulatory requirement. Under CMS Memo QSO-24-08-NH, effective April 1, 2024, any resident with a chronic wound or indwelling medical device must be placed on EBP.
Staff performing high-contact care activities — dressing, bathing, transferring, changing linens, wound care, device care — must wear gown and gloves regardless of whether the resident has a confirmed MDRO. EBP applies even when Contact Precautions are not otherwise indicated.
Staff Immunization
PPE alone doesn't close every transmission gap — staff vaccination is an equally critical layer. CDC MMWR data from the 2024–25 influenza season reported 42.1% vaccination coverage among nursing home healthcare workers, down from 45.4% the prior season. For a resident population with limited immune reserves, that gap is consequential.
ACIP recommends annual influenza vaccination for all healthcare personnel without contraindications. Facilities that cannot mandate vaccination should take several steps to reduce exposure:
- Require unvaccinated staff to wear surgical masks throughout flu season when around residents
- Track and report vaccination rates as part of the facility's IPC program
- Offer on-site vaccination clinics to reduce access barriers for staff
Resident Placement, Isolation, and Space Configuration
Prioritizing Private Rooms
When a resident has an airborne infection, draining wound, or uncontained secretions, a private room is the first-line response. CDC transmission-based precaution guidance supports this, and multisociety nursing home IPC guidance (2024) recommends private-room isolation with the door closed while awaiting transfer when a dedicated airborne infection isolation room (AIIR) is unavailable — since most LTCFs simply don't have negative-pressure rooms.
When private rooms aren't available, cohorting — placing residents with the same confirmed pathogen together in a shared space — is the next best approach. Assigning a dedicated cohort of staff to those residents further limits cross-exposure.
Signage and Communication
Every resident under transmission-based precautions should have clear, standardized signage posted outside their room. CDC provides standardized contact, droplet, and airborne precaution signage for exactly this purpose. For residents under EBP, signage should specify which care activities trigger gown and glove use, since EBP doesn't require those precautions for all contact — only for high-contact care activities.
The Infrastructure Gap — and a Practical Solution
Most LTCFs were not designed with flexible isolation capacity in mind. A survey cited in SHEA/APIC guidelines found that while 90.5% of LTCFs accepting MRSA-positive residents reported following Contact Precautions, only 39.7% placed those residents in private rooms. The gap reflects a real-world constraint: shared rooms, communal hallways, and the home-like environment residents depend on don't always accommodate traditional isolation approaches.
Portable, retractable privacy screens — such as Rolascreen's Portable Elite models — give facilities a flexible, no-construction option for separating residents in shared rooms or common areas. Key features that support IPC workflows:
- Wipe-clean surfaces: Non-porous medical-grade polyester film panels disinfect with the same EPA-registered hospital disinfectants used on bedrails and high-touch surfaces
- Terminal cleaning integration: Panel disinfection fits directly into existing room-turnover protocols without additional steps
- Repositionable design: When an outbreak resolves or cohorting needs shift, screens relocate easily or nest compactly for storage

HVAC as a Supporting Layer
Physical barriers address resident-to-resident exposure at the room level. Environmental controls operate at a different scale — and both matter. Air quality supports, but doesn't replace, physical separation. Facilities should know their HVAC filter ratings (CDC recommends MERV-13 or higher when possible) and ensure systems are serviced regularly. The Florida AJIC needs assessment found that infection preventionists had limited awareness of their facility's HVAC scope — a finding that points to ventilation knowledge as a genuine training gap in LTCF IPC programs.
Outbreak Management, CMS Compliance, and Staff Training
Outbreak Preparedness Protocols
An effective outbreak management plan addresses more than the clinical response. Key components include:
- Physical distancing strategies in communal dining rooms and activity spaces
- Visitor and staff symptom screening at entry points
- Defined testing and treatment protocols for identified pathogens
- Communication plans for residents, families, and referring hospitals
- PPE and disinfectant supply chain continuity
- Cross-trained staffing to manage coverage during surge
CDC's Viral Respiratory Pathogens Toolkit for Nursing Homes provides a structured framework organized around preparation and active response — including vaccination, ventilation, cohorting, health department notification, and testing protocols.
IPC Staff Training and Monitoring
Training quality matters as much as training frequency. Evidence-based approaches for LTCFs include:
- Mandatory IPC training at hire and annually
- Return demonstration of hand hygiene technique and PPE donning/doffing
- Direct observation audits for hand hygiene compliance
- Regular infection control roundtables where frontline staff can surface gaps
A Florida AJIC survey found that 81% of infection preventionists with that as their sole title had 5 or fewer years of IPC experience. A national survey found that 61% of infection control professionals in nursing homes had no specific IPC training at all.
These numbers make ongoing mentorship and professional development programs a structural necessity, not an afterthought.
That accountability extends to the regulatory level. Under 42 CFR 483.75, CMS requires the Quality Assurance and Performance Improvement committee to include at least one infection preventionist and meet at minimum quarterly. IPC metrics should be a standing agenda item, not a periodic add-on.
Frequently Asked Questions
What are the infection control measures in care homes?
Core measures span several areas: hand hygiene before and after resident contact, PPE matched to each exposure type, disinfection of high-touch surfaces, isolation or cohorting when indicated, staff immunization, and active surveillance for infections and MDROs. CMS-required antibiotic stewardship and ongoing staff training complete the program.
What are the 5 principles of infection control?
The five principles are: (1) surveillance and detection, (2) standard and transmission-based precautions, (3) hand hygiene, (4) environmental cleaning and disinfection, and (5) antibiotic stewardship. All five carry added weight in long-term care, where close proximity and compounding resident risk factors accelerate transmission.
What is the most common infection in long-term care facilities?
UTIs are the most frequently reported infection type, followed by respiratory infections (pneumonia, influenza) and skin/soft tissue infections. MDRO colonization is prevalent in an estimated 50% or more of the nursing home population, creating ongoing transmission risk even among residents without active symptoms.
What does CMS require for infection prevention in long-term care?
The 2016 CMS final rule (42 CFR 483.80) requires a formal IPCP, a designated infection preventionist working at least part-time, and an antibiotic stewardship program with protocols and monitoring. The 2024 update (F880 / QSO-24-08-NH) added Enhanced Barrier Precautions as a mandatory standard, effective April 1, 2024.
What are Enhanced Barrier Precautions (EBP) in nursing homes?
EBP requires staff to wear gown and gloves during high-contact care activities — including dressing, bathing, transferring, linen changes, and wound care — for any resident with a chronic wound or indwelling medical device. This applies regardless of confirmed MDRO status. Residents under EBP are not room-restricted and may continue participating in group activities.