Introduction
On any given day, roughly 1 in 31 hospitalized patients in the U.S. has at least one healthcare-associated infection — amounting to an estimated 687,000 HAIs annually and 72,000 deaths during affected hospitalizations. The direct medical costs to U.S. hospitals run between $28.4 billion and $45 billion per year.
What makes these numbers particularly frustrating is that most HAIs are preventable. Evidence-based protocols exist. Staff know the guidelines. Yet infections persist — not because healthcare workers lack knowledge, but because systemic barriers get in the way of consistent practice.
Infection prevention and control (IPC) refers to the evidence-based practices that reduce pathogen transmission in healthcare settings. Those barriers tend to cluster into four categories: gaps in staff training, organizational culture problems, physical facility constraints, and patient behavioral factors. Left unaddressed, each one compounds the others — driving HAI rates higher than any single intervention can fix alone.
This article breaks down each barrier category and outlines practical, low-disruption solutions — from protocol redesign to physical environment changes — that facilities can put into action without overhauling their entire operation.
Key Takeaways
- IPC barriers span individual, organizational, and environmental levels — and effective solutions must address all three
- Training gaps and high workloads are the most frequently documented reasons for IPC non-compliance
- Leadership behavior and organizational culture shape whether IPC is a daily norm or a paper exercise
- Open floor plans and shared spaces create hidden infection transmission risks that protocols alone can't solve
- Practical solutions exist for every barrier category, from peer coaching models to non-porous physical partitioning
Why IPC Barriers Matter in Healthcare Settings
The scale of the problem gives context for why barriers matter. The CDC's hospital prevalence survey found 687,000 HAIs in U.S. acute care hospitals in a single year, with 72,000 deaths during hospitalizations where HAIs were present. Adjusted for inpatient hospital service prices, the annual cost to hospitals reaches up to $45 billion.
When IPC protocols break down, healthcare workers face direct occupational exposure — needlestick injuries, respiratory pathogen exposure, and contact transmission from improperly managed patients. That creates a dual safety imperative: HAI prevention protects patients and the clinical workforce.
IPC failures aren't simply a matter of individual non-compliance. They operate at three distinct levels:
- Micro level — individual HCW knowledge, habits, and workload
- Meso level — facility culture, leadership, and resource allocation
- Macro level — physical infrastructure and system design
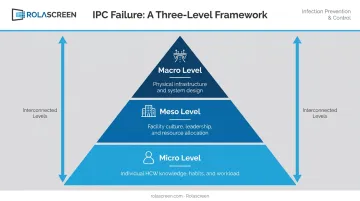
Effective IPC programs must address all three levels simultaneously. A facility that improves hand hygiene compliance while leaving chronic understaffing or open ward layouts unaddressed is solving only a fraction of the problem.
Staff Training and Workload-Related Barriers
The Knowledge-Practice Gap
Training gaps are among the most consistently documented IPC barriers. A 2021 systematic review found that in one U.S. study, 20.8% of healthcare workers had not received hand hygiene training or orientation in the prior year. That's roughly 1 in 5 active clinical staff without recent formal IPC instruction.
The more stubborn problem, though, isn't absence of training: it's the gap between knowing and doing. A 2025 AJIC study at two U.S. hospitals found nurses and physicians self-reported hand hygiene adherence above 90%, while direct observation showed actual compliance at 46.2%.
That's nearly a 45-percentage-point gap between perceived and actual practice — a finding that challenges the assumption that awareness alone drives behavior.
Workload as a Competing Priority
High patient-to-staff ratios directly erode IPC compliance. Research published in Infection Control & Hospital Epidemiology found hand hygiene compliance held near 40% until workload exceeded 30 opportunities per hour — after that, compliance dropped by approximately one percentage point for each additional opportunity per hour. When staff are already stretched, IPC steps become the first things cut under time pressure.
Guideline Overload and Staff Turnover
Two more barriers compound the training problem:
- Protocol fatigue: A 2020 Cochrane qualitative evidence synthesis found HCWs reported IPC guidelines were often lengthy, ambiguous, and inconsistently aligned with national guidance. Excluding support staff (cleaners, porters) from training programs was also a documented gap.
- New employees who haven't completed IPC orientation represent a continuous vulnerability — onboarding programs that treat IPC as secondary to clinical skills leave compliance gaps in the first critical weeks of employment.
Organizational and Leadership Barriers to IPC
Leadership Accountability and Culture
IPC programs require governance-level ownership, not just goodwill. CDC Core Practices explicitly require that the governing body of a healthcare facility be accountable for the success of infection prevention activities, with adequate human and material resources allocated accordingly. When facility leadership doesn't visibly prioritize IPC through budget decisions and accountability structures, programs remain underfunded and deprioritized.
Culture matters just as much as policy. Facilities where IPC is treated as a compliance checkbox see markedly lower adherence than those where infection control is embedded in daily team norms and peer accountability is normalized. Leadership has to model the behavior first — policy alone won't move the culture.
Staffing and Resource Gaps
The numbers on infection prevention (IP) staffing are telling. A 2024 AJIC study of 390 hospitals found that 79.2% had IP staffing levels below recommended benchmarks — with median staffing at 1 IP FTE per 121 beds, against a recommended ratio closer to 1 per 69 beds. Facilities below expected staffing had significantly higher HAI rates: 25% of under-staffed facilities showed elevated CAUTI rates versus 7% of adequately staffed ones.
Resource gaps compound the staffing problem:
- Insufficient hand hygiene stations at point-of-care
- PPE that isn't readily accessible when and where it's needed
- Absent spill kits or limited disinfectant supplies in clinical areas
- No designated IPC lead in smaller or resource-constrained facilities

Missing Feedback Loops
Understaffed programs also tend to lack the bandwidth for consistent monitoring. Without regular audits, surveillance data, and transparent reporting back to clinical staff and leadership, IPC problems stay invisible until an outbreak forces a response. The absence of structured performance monitoring — not just collecting data, but acting on it and sharing results — is one of the most common reasons well-designed IPC programs stall after initial implementation.
Physical Environment and Facility Design Barriers
When Layout Works Against You
The physical structure of a healthcare facility can undermine IPC regardless of how well-trained the staff are. Open ward designs, multi-bed rooms, and shared waiting areas make it structurally difficult to separate patients with suspected or confirmed infections from others.
CDC isolation guidance recommends single-patient rooms for patients requiring Contact or Droplet Precautions, and where multi-patient rooms are unavoidable, at least 3 feet of spatial separation between beds. A 2024 systematic review and meta-analysis confirmed the stakes: single-patient ICU rooms significantly reduced nosocomial infection rates (OR 0.68) and MDRO acquisition (OR 0.41) compared to multi-patient configurations. The physical environment is an active variable in transmission risk, not just a backdrop.
The Fabric Curtain Problem
Standard fabric privacy curtains are a commonly overlooked IPC liability. A longitudinal AJIC study found 92% of hospital privacy curtains were contaminated within one week of laundering. Fabric is porous, can't withstand aggressive disinfectants, and is practically excluded from terminal cleaning workflows — meaning the surface closest to every patient bed is regularly harboring pathogens that no cleaning protocol addresses.

Facilities commonly resort to pulling chairs together or posting temporary signage, neither of which creates a meaningful physical barrier or supports disinfection between uses.
Rolascreen's portable wheeled screens address this directly. The nesting form factor allows clinical teams to convert non-clinical spaces into infection-controllable bays in minutes, with screens that retract for compact storage between uses.
They've been deployed across a range of high-acuity environments, specifically because they meet the disinfection standards those settings require without facility modification:
- ED triage bays requiring rapid patient cohorting
- Contact precaution rooms needing cleanable barriers
- Airborne isolation environments during outbreak responses
- Surge overflow areas where no permanent infrastructure exists
Patient and Behavioral Barriers to Infection Control
Patient non-compliance with IPC measures — respiratory hygiene, hand hygiene, staying in designated areas — is a genuine challenge for clinical staff. It's particularly pronounced when patients have cognitive impairments, language barriers, or limited health literacy.
A 2025 systematic review found pooled hand hygiene compliance among hospital visitors was only 37% — 43% in ICUs and 29% in medical/surgical wards. Patients, families, and caregivers are part of the transmission chain, and gaps in their compliance directly increase transmission risk.
CDC Core Practices include patient, family, and caregiver education as a required IPC component, not an optional enhancement. When patients and families understand why a measure is in place — not just that they're supposed to follow it — compliance improves.
A 2023 ICHE article noted that approximately 8% of the U.S. population has limited English proficiency, creating a structural barrier to IPC instruction that interpreter access alone doesn't fully solve.
These barriers aren't isolated — they tend to cluster around the same patient populations. Common factors that reduce compliance include:
- Cognitive impairment or dementia limiting ability to follow instructions
- Limited English proficiency with no available interpreter
- Low health literacy leaving patients unclear on the purpose of precautions
- Discomfort or anxiety in open, poorly partitioned spaces
Communication barriers and environmental design are more connected than they appear. Patients who feel exposed or uncomfortable in open, poorly partitioned spaces are less cooperative with infection control measures overall. Proper physical partitioning reduces pathogen transmission and supports patient dignity — and patients who feel respected are more willing to follow the precautions being asked of them.
Practical Strategies to Overcome IPC Barriers
Staff and Training Interventions
- Structured onboarding — IPC orientation on day one, with role-specific practical content rather than generic facility-wide modules
- Annual refreshers — Simulation-based training shows measurable improvements in practical IPC skills; online modules alone are insufficient
- Peer coaching — Designating experienced staff as IPC champions normalizes accountability without relying solely on top-down enforcement
- Context-specific guidelines — Protocols simplified for the specific unit, so staff can act quickly rather than search through facility-wide documents
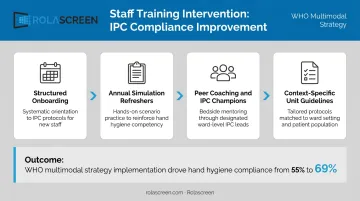
WHO's multimodal hand hygiene strategy — combining system change, training, evaluation/feedback, reminders, and institutional safety climate — improved overall compliance from 55% to 69% in pilot implementation.
Organizational and Leadership Actions
- Assign a dedicated infection control professional with clear accountability, not fragmented responsibility across roles
- Build performance monitoring into regular leadership reviews — not just annual reports
- Ensure PPE and cleaning supplies are stocked at point-of-care, not in a supply room down the hall
- Make IPC audit results visible to clinical teams, not just administration
Research on hand sanitizer placement is concrete: a 2015 AJIC study across 12 inpatient units found that dispenser visibility and room-entry accessibility were significantly associated with higher hand hygiene compliance — with overall compliance reaching 81.6% in well-configured environments.
Environmental and Physical Solutions
A facility space audit surfaces the most actionable gaps. Key questions:
- Where are the highest-traffic zones with shared surfaces?
- Which areas have open layouts that make patient separation structurally difficult?
- Are current privacy curtains replaced on a schedule that accounts for contamination rates?
For facilities addressing the physical environment without construction, two practical, non-construction upgrades stand out: replacing porous fabric curtains with non-porous alternatives, and introducing flexible partitioning for surge capacity.
Rolascreen's retractable screens — in portable wheeled and wall-mounted configurations — use non-porous medical-grade film panels that wipe down with EPA-registered hospital disinfectants between patients, fitting into existing cleaning workflows. Rolascreen also offers a consultation service to help facilities identify high-risk placement areas before committing to purchases.
Frequently Asked Questions
What are the barriers to infection prevention and control in a healthcare setting?
The main categories are staff training gaps, high workloads, organizational and leadership deficiencies, inadequate PPE and supplies, physical facility design limitations, and patient behavioral factors. Effective IPC requires addressing barriers at multiple levels simultaneously — targeting only one rarely produces sustained improvement.
What are the 5 F's of infection control?
The 5 F's refer to key fecal-oral transmission routes used in public health: Fingers, Flies, Food, Fluids, and Fields (or Fomites in some framings). The framework pinpoints where hygiene and environmental controls must be applied to break the chain of transmission.
What is the most common barrier to infection control in hospitals?
Studies point to lack of formal IPC training and high workload or time pressure as the most frequently reported barriers, followed closely by insufficient access to PPE and supplies at the point of care.
How does understaffing affect infection prevention and control?
Understaffing increases workload per worker, leaving less time to follow IPC protocols such as proper gloving and disinfecting between patients. It also slows environmental cleaning turnaround and limits compliance monitoring.
What role does the physical environment play in healthcare-associated infections?
Open floor plans, shared spaces, and porous or hard-to-clean surfaces all increase pathogen transmission risk. Physical design that supports patient separation, easy surface disinfection, and minimal clutter is an underappreciated component of effective IPC programs.
How can healthcare facilities improve IPC compliance among staff?
Effective approaches combine role-specific training, visible leadership commitment, peer accountability, and supplies available at the point of care. Multifaceted strategies that address behavior, culture, and environment together outperform single-intervention approaches.