Introduction
Hospital-acquired pneumonia made up 25.8% of all HAIs in a 2023 point-prevalence survey of 218 U.S. acute care hospitals — and each case adds 8.3 extra hospital days with a 13.1% mortality rate, according to a 2024 case-control study. Respiratory infections aren't a background risk. They're one of the leading drivers of preventable harm.
Those numbers translate directly into operational pressure. Longer stays mean higher liability exposure, strained capacity, and added burden on already-stretched infection control teams. A 2024 APIC report found that nearly 4 in 5 U.S. hospitals lack sufficient infection prevention staffing — making every protocol gap more costly.
Airborne pathogens like Mycobacterium tuberculosis, measles, and varicella add another layer of complexity. Controlling them requires engineering controls, ventilation strategy, clinical protocols, PPE discipline, and staff training working in concert — no single measure is sufficient alone. This article breaks down each of those layers: what the evidence says, where facilities commonly fall short, and what it takes to get each one right.
Key Takeaways
- Airborne precautions supplement standard precautions — they don't replace hand hygiene, gowns, or gloves
- Fit-tested N95 respirators (or PAPRs) are mandatory for airborne isolation rooms; surgical masks are not equivalent
- AIIRs must maintain negative pressure with 6–12 air changes per hour, exhausting air outside or through HEPA filtration
- Without an AIIR: mask the patient, close the door, and initiate transfer — interim steps reduce but don't eliminate risk
- Ventilation, PPE compliance, and staff protocols require ongoing monitoring — not one-time setup
Understanding Airborne Transmission in Healthcare Settings
How Airborne Transmission Works
Airborne transmission occurs through droplet nuclei — particles ≤5 micrometers in diameter that remain suspended in air, travel across rooms, and can move through ventilation systems. This is distinct from larger respiratory droplets, which fall quickly and require only close-contact precautions.
The difference matters clinically. A patient with influenza a few feet away is a droplet risk. A patient with active pulmonary TB in an adjacent room with shared HVAC airflow is an airborne risk — the particle physics are fundamentally different, and so are the required controls.
Pathogens That Require Airborne Precautions
Per CDC Appendix A, four conditions specifically require airborne precautions in healthcare settings:
- Tuberculosis (M. tuberculosis) — pulmonary or laryngeal disease
- Measles (rubeola)
- Varicella (chickenpox) — combined with contact precautions
- Disseminated herpes zoster — and localized zoster in immunocompromised patients until dissemination is ruled out
These pathogens are not governed by droplet precautions. They require dedicated room environments, specialized PPE, and entirely separate patient management protocols.
Why Healthcare Settings Amplify Risk
The built environment itself creates vulnerabilities:
- Multi-bed wards share airspace across multiple patients simultaneously
- Recirculated HVAC air can distribute particles throughout a unit if filtration is inadequate
- Patient transport through corridors creates transient exposure in shared spaces
- High concentrations of immunocompromised patients face elevated susceptibility even at low infectious doses
A Canadian hospital study found that tuberculin conversion among healthcare workers was strongly associated with inadequate ventilation in general patient rooms — not in dedicated respiratory isolation rooms. That finding has a direct policy consequence: general ward ventilation standards deserve the same scrutiny as formal isolation room specifications.
Airborne Infection Control Guidelines for Healthcare Facilities
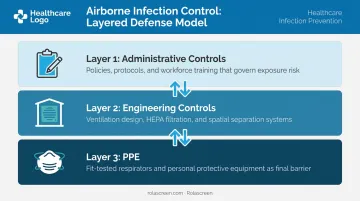
Effective airborne infection control depends on three interdependent layers: administrative controls (policies and protocols), engineering controls (room design and ventilation), and PPE. A gap in any one layer increases transmission risk for staff and other patients.
General Precautions and PPE Requirements
Airborne precautions are added on top of standard precautions — not in place of them. Hand hygiene, gowns, and gloves remain required. What changes is respiratory protection and room environment.
For healthcare personnel entering an airborne isolation room:
- Wear a fit-tested, NIOSH-approved N95 respirator or a Powered Air-Purifying Respirator (PAPR)
- Don the respirator before entering and remove it only after fully exiting
- Perform a user seal check each time before putting on an N95
- Complete fit testing before initial use and repeat at least annually per OSHA requirements
For the patient:
- Wear a procedure or surgical mask whenever outside the isolation room
- Follow respiratory hygiene and cough etiquette
- Avoid shared spaces and close contact with others during transport
Setting Up and Using Airborne Infection Isolation Rooms (AIIRs)
AIIR engineering requirements per CDC guidance:
| Requirement | Existing Facilities | New Construction/Renovation |
|---|---|---|
| Air pressure | Negative (2.5 Pa / 0.01 in. water gauge relative to corridor) | Same |
| Air changes per hour | Minimum 6 ACH | Minimum 12 ACH |
| Exhaust | Directly outside or HEPA-filtered before any recirculation | Same |
Pressure must be monitored continuously using manometers, smoke tubes, or flutter strips. Sealed windows and self-closing doors are required — every time a door opens without a vestibule, there's potential for contaminated air to escape into the corridor.
Room clearance after patient discharge:
At 6 ACH, CDC data shows 46 minutes for 99% particle removal and 69 minutes for 99.9% removal. At 12 ACH, those times drop to 23 minutes and 35 minutes, respectively. The appropriate wait time depends on your facility's actual ACH rate — a blanket "one-hour rule" isn't accurate across all settings.
Patient Placement and Movement Protocols
- Use a single-patient AIIR whenever available
- Limit movement outside the AIIR to medically necessary purposes only
- During transport, the patient wears a surgical mask — healthcare personnel transporting a masked patient generally do not need to wear a respirator if infectious lesions are also covered
- In acute care settings without an available AIIR, mask the patient immediately, place them in a private room with the door closed, and initiate transfer protocols
Interim Measures When an AIIR Is Unavailable
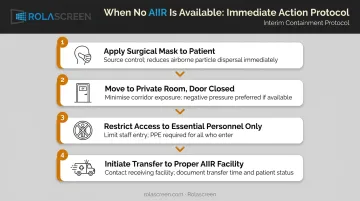
When a dedicated AIIR isn't immediately accessible, activate these steps without delay:
- Apply a surgical mask to the patient as source control
- Move the patient to a private room with the door closed — this reduces but does not eliminate spread
- Restrict room access to essential personnel only
- Contact a facility with proper airborne isolation capacity and initiate transfer immediately
Physical separation in open spaces — ED waiting areas, multi-patient holding bays, triage corridors — is a critical interim layer. Direct suspected airborne infection patients away from general waiting areas and separate them from others using visual and physical barriers.
Healthcare facilities increasingly use portable retractable privacy screens with non-porous, wipeable surfaces to quickly reconfigure open spaces for interim separation without permanent construction. Rolascreen's Portable Elite screens, for example, deploy without tools and extend up to 123 inches wide — enough to partition an ED bay or multi-patient holding area within minutes.
Their medical-grade polyester film surfaces are compatible with EPA-registered hospital disinfectants, including bleach, quaternary ammonium compounds, and accelerated hydrogen peroxide.
Physical barriers and source control address immediate exposure risk, but they are stop-gap controls only. The goal must always be proper AIIR placement as quickly as possible.
HVAC Systems and Environmental Air Controls
What a Properly Functioning HVAC System Must Do
In airborne infection control, the HVAC system functions as a primary clinical control — not a passive building feature. It must:
- Maintain correct pressure differentials in AIIRs and protective environments
- Deliver the required ACH consistently, including during peak occupancy
- Pass air through appropriate filtration (HEPA for isolation and protective environments)
HVAC failure has consequences. A 2015 review in Clinical Infectious Diseases identified 53 healthcare fungal outbreaks during construction and renovation between 1974 and 2014, with Aspergillus as the most common pathogen. Inadequate ventilation has also caused TB transmission to healthcare workers.
Supplemental Air-Cleaning Measures
When central systems are inadequate or under maintenance, supplemental measures include:
- HEPA filtration — at minimum 99.97% efficient for particles ≥0.3 micrometers
- Portable HEPA units — should achieve ≥12 ACH when deployed; do not satisfy fresh-air requirements
- Ultraviolet Germicidal Irradiation (UVGI) — a supplemental adjunct in upper-room or duct-system applications; not a substitute for negative pressure or HEPA filtration
- Portable industrial HEPA units — practical for providing equivalent ACH when permanent systems are temporarily compromised
Supplemental measures address gaps in existing systems. Preventing those gaps from occurring in the first place — particularly during construction — requires its own protocol.
Construction and Renovation Risk
Demolition disturbs fungal spores and aerosolizes pathogens. Before any construction or renovation project, facilities must:
- Conduct an Infection Control Risk Assessment (ICRA)
- Establish physical dust barriers with negative pressure in the construction zone
- Increase HVAC monitoring frequency during and after the project
- Restrict immunocompromised patients from areas adjacent to active construction
Common Airborne Infection Control Mistakes to Avoid
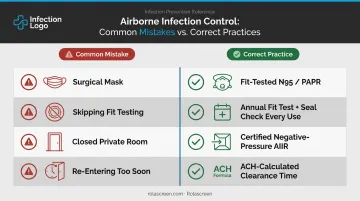
1. Using a surgical mask instead of an N95 A surgical mask does not create a tight facial seal and cannot filter particles at the level required for airborne pathogens. One N95 compliance study cited in CDC/HICPAC draft appendices found compliance rates as low as 40.6% — a significant gap given what's at stake for staff and patients alike.
2. Skipping fit testing or the pre-use seal check An N95 that hasn't been properly fit-tested offers false protection. Staff may believe they're protected while airborne particles bypass the mask seal. OSHA requires:
- Initial fit testing before first use
- Annual retesting at minimum
- A seal check every single time the respirator is donned
3. Treating a closed-door private room as equivalent to an AIIR A standard room with a closed door reduces airborne spread, but it does not eliminate it. Without consistent negative pressure relative to the hallway, contaminated air escapes each time the door opens.
Studies show that door motion and foot traffic drive measurable airflow across isolation-room doorways even when the room is technically maintaining negative pressure.
4. Re-entering a room before adequate clearance time Entering too soon after an airborne-precaution patient vacates — before sufficient air changes have cleared the room — exposes the next occupant to the same risk as being present with the patient. Clearance time must be calculated based on the room's actual ACH rate, not assumed to be one hour across all settings.
Conclusion
No single measure controls airborne transmission in healthcare. N95 respirators without proper AIIRs leave staff exposed. Negative-pressure rooms without fit-tested PPE leave gaps at the staff level. Without protocol adherence, even the best HVAC systems fail at the behavioral level.
Effective airborne infection control is a systems discipline: administrative protocols, engineering controls, and staff behavior operating together, consistently. Treat it as an ongoing operational standard — not a response triggered by outbreaks.
To stay ahead of risk, build these into regular operations:
- Schedule HVAC audits at defined intervals
- Maintain fit-testing calendars for all staff using respirators
- Review isolation protocols annually
- Assess the physical environment before problems surface
Outbreak response is reactive by definition. Prevention is not.
Frequently Asked Questions
What are airborne precautions in healthcare?
Airborne precautions are infection control measures applied in addition to standard precautions for patients known or suspected to carry diseases transmitted via droplet nuclei — including TB, measles, and varicella. They cover specific PPE requirements, dedicated room environments, and patient management protocols to prevent pathogen spread.
What are the CDC guidelines for airborne precautions?
CDC guidance calls for placement in a negative-pressure AIIR with 6–12 ACH (minimum), use of fit-tested N95 respirators or PAPRs by healthcare personnel, surgical masking of patients during transport, and restriction of susceptible staff from entering rooms of high-risk patients when immune staff are available.
What PPE is required for a patient on airborne precautions?
Healthcare workers must wear a fit-tested N95 respirator or PAPR — donned before entry, removed after exiting. Standard precaution PPE (gloves and gown) remains in place. The patient must wear a surgical mask whenever outside the isolation room.
What diseases require airborne precautions in a healthcare setting?
The four primary conditions are tuberculosis (M. tuberculosis), measles (rubeola), varicella (chickenpox), and disseminated herpes zoster — as well as localized zoster in immunocompromised patients until dissemination is ruled out.
What is an Airborne Infection Isolation Room (AIIR)?
An AIIR is a specially engineered single-patient room that maintains negative air pressure relative to surrounding areas (2.5 Pa / 0.01 in. water gauge) and provides a minimum of 6–12 ACH depending on facility type. Air exhausts directly outside or through HEPA filtration to prevent contaminated air from escaping into the rest of the facility.
How long should a room remain vacant after an airborne precaution patient leaves?
The wait time depends on the room's ACH rate. At 6 ACH, CDC data indicates 46 minutes for 99% particle removal and 69 minutes for 99.9%. At 12 ACH, those times drop to 23 and 35 minutes, respectively.