Introduction
According to the CDC, 1 in 31 U.S. hospital patients has at least one healthcare-associated infection (HAI) on any given day. Tens of thousands of patients with HAIs die during their hospitalizations each year. AHRQ estimates HAIs cost the healthcare system between $28 billion and $33 billion annually in excess costs.
Those numbers carry direct operational consequences. CMS's Hospital-Acquired Condition Reduction Program applies a 1% Medicare payment reduction to hospitals in the worst-performing quartile. The Joint Commission's 2024 standards updates have also shifted survey focus from paperwork to on-the-ground implementation — accreditation risk is real and measurable.
Hand hygiene gets most of the attention. But the physical environment — surfaces, furnishings, spatial layout, air, and the materials dividing patient spaces — is an equally significant transmission vector, and one that facilities consistently underestimate. This guide covers what CDC, Joint Commission, CMS, and OSHA require, and where facilities most often fall short.
Key Takeaways
- 1 in 31 hospital patients has an HAI on any given day — the physical environment is a documented contributor when cleaning protocols fail
- The CDC's six core components and The Joint Commission's 2024 IC standards set the baseline compliance framework
- Cleaning must always precede disinfection — applying germicide to soiled surfaces is one of the most common and preventable failure points
- Disinfectant selection must match both the surface and the pathogen — standard quaternary ammonium products cannot kill C. difficile spores
- Porous materials like fabric privacy curtains cannot be disinfected by wiping — making them an ongoing and underestimated HAI risk
Understanding Environmental Infection Control in Healthcare
Environmental infection control covers how the physical healthcare environment — surfaces, air, water, and spatial layout — is actively managed to prevent pathogen transmission to patients, staff, and visitors. It spans cleaning protocols, disinfection product selection, air and water management, and spatial layout. Multiple regulatory bodies govern different pieces of this discipline:
| Authority | What They Govern |
|---|---|
| CDC | Technical guidelines for environmental cleaning, disinfection, and EVS practices |
| The Joint Commission | Accreditation standards, including the 2024 IC chapter update |
| CMS | Medicare/Medicaid Conditions of Participation (42 CFR 482.42) |
| OSHA | Worker safety during cleaning (Bloodborne Pathogens Standard, 29 CFR 1910.1030) |
These agencies are not redundant. A facility can satisfy CMS CoPs while still failing a Joint Commission survey, or maintain compliant EVS protocols while exposing housekeeping staff to OSHA violations. Compliance requires all four lanes.
The CDC's Six Core Components
CDC's 2024 surface-risk guidance organizes environmental cleaning around six core components. A gap in any single component increases facility-wide infection risk:
- Integrate environmental services into the facility's safety culture
- Educate and train all personnel responsible for cleaning and disinfection
- Select appropriate cleaning and disinfection technologies and products
- Standardize setting-specific cleaning and disinfection protocols
- Monitor effectiveness and adherence to protocols
- Provide feedback on cleaning adequacy to staff and stakeholders
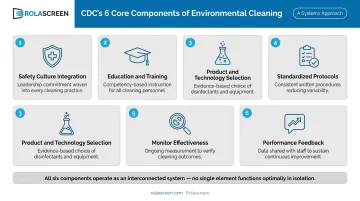
These components work as a system, not a menu. A facility with excellent product selection but no monitoring program carries a compliance gap — and survey teams will find it.
Surface Cleaning and Disinfection Protocols
Cleaning must always precede disinfection. This is a foundational CDC requirement, not a procedural preference. Organic matter, salts, and visible soil interfere with microbial inactivation. Applying a disinfectant to an uncleaned surface can render it chemically ineffective regardless of the product's EPA registration.
A 2022 study found that only 40–50% of high-touch surfaces were consistently cleaned at baseline, and sustained improvement to over 90% cleaning adherence was associated with 75% lower overall HAI rates and 70% lower C. diff acquisition over 10 years. The cleaning step is where most programs fail.
Understanding Disinfection Levels
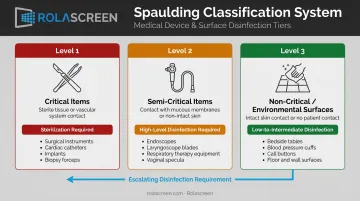
The Spaulding Classification system provides the CDC-endorsed framework for determining required disinfection levels:
- Critical items (enter sterile tissue or vascular system) → Sterilization required
- Semi-critical items (contact mucous membranes or non-intact skin) → High-level disinfection at minimum
- Non-critical items (contact intact skin only) → Low-level disinfection
- Environmental surfaces (floors, walls, countertops, equipment exteriors) → Routine low- or intermediate-level disinfection using EPA-registered hospital disinfectants
EPA-registered hospital disinfectants are products demonstrated effective against Staphylococcus aureus, Salmonella enterica, and Pseudomonas aeruginosa. Products without a tuberculocidal claim are classified as low-level disinfectants; those with one qualify as intermediate-level.
Using unregistered products creates both liability and compliance exposure. Not following EPA label conditions — dilution, contact time, application method — is a federal FIFRA violation.
Selecting the Right Disinfectant
Disinfectant selection depends on four factors:
- Surface porosity and material — hard non-porous surfaces vs. textiles require different approaches
- Pathogen concern — C. diff spores require EPA List K sporicidal products; standard quats don't qualify
- Manufacturer compatibility — medical equipment labels often specify approved disinfectants
- OSHA/SDS requirements — staff handling requirements vary by chemical class
Quaternary ammonium compounds (quats) are among the most widely used hospital disinfectants — but they are generally not sporicidal. One hospital study found that switching from quat products to unbuffered hypochlorite in C. diff patient rooms was associated with CDAD rates dropping from 8.6 to 3.3 cases per 1,000 patient-days.
EPA List K currently includes 94 registered products effective against C. diff spores — sodium hypochlorite, hydrogen peroxide, peroxyacetic acid, and chlorine-releasing compounds among them.
Disinfectant choice is only part of the equation. Cleaning equipment itself becomes a contamination source when not managed properly. CDC guidance specifies that mop heads and cleaning cloths should be changed when visibly soiled, always after use in isolation areas, and should never be left soaking in dirty bucket solutions. Reusable cloths must be laundered and dried before reuse. A dirty mop transfers pathogens rather than removing them.
Managing High-Touch Surfaces and Physical Environments
Not all surfaces carry equal transmission risk, and CDC's environmental cleaning guidance reflects that directly. The framework is risk-stratified:
- High-touch surfaces (bedrails, doorknobs, light switches, IV poles, call buttons, bathroom fixtures) — cleaned and disinfected more frequently, at minimum daily in occupied patient areas
- Low-touch surfaces (floors, ceilings, window sills) — regular wet mopping with detergent/water under normal conditions
CDC is explicit that extraordinary floor disinfection offers no additional benefit over standard wet mopping in routine settings. Floor disinfectant use isn't required for infection control purposes — though facilities often apply it anyway when they can't distinguish routine dirt from body fluid contamination.
High-Touch vs. Low-Touch Surface Protocols
For surfaces that are frequently touched but difficult to clean — equipment controls, handles, panel surfaces — CDC recommends barrier protection strategies: non-porous covers such as plastic wrap, aluminum foil, or fluid-resistant barriers that are removed and replaced between patients or when visibly soiled.
Contact-precaution rooms require prioritized and more frequent cleaning — at least daily — with terminal cleaning and disinfection required upon every patient discharge or transfer.
Joint Commission's 2024 updates have shifted survey methodology from documentation review to practical verification, meaning surveyors are now more likely to observe actual EVS practice than simply audit paperwork.
Carpets, Curtains, and Cloth Furnishings
Porous materials in patient-care environments present a compliance problem that hard-surface protocols cannot solve:
- Carpeting harbors gram-negative bacteria and fungi, particularly when damp — CDC recommends avoiding it in ICUs, burn units, ORs, and HSCT units
- Upholstered furnishings cannot be fully decontaminated after body fluid exposure — CDC advises against them near immunosuppressed patients
- Fabric privacy curtains represent a frequently overlooked high-touch surface that cannot be wiped with hospital-grade disinfectants
The evidence on curtain contamination is consistent. A longitudinal study (Shek et al., 2018) found MRSA on freshly laundered curtains as early as day 10, with 5 of 8 test curtains positive by day 14. Earlier research (Trillis et al., 2008) found 42% VRE and 22% MRSA on sampled hospital curtains, with organisms transferable by hand contact. In a separate study (Ohl et al., 2012), 95% of 43 curtains were contaminated at least once — some within the first week.

The core problem: EPA's registered hospital disinfectants and List K sporicidal products are validated for hard, non-porous surfaces. A standard hospital disinfectant cannot be applied to a fabric curtain and produce a compliant disinfection outcome unless the product label specifically supports soft-surface use — which most do not.
Rolascreen's retractable privacy screens use thermally-stabilized medical-grade polyester film panels — non-porous — that can be wiped down with hospital-grade disinfectants including bleach at concentrations up to 10,000 ppm, which exceeds the CDC's 5,000 ppm sporicidal threshold for C. difficile.
An optional antimicrobial finish (tested to ISO 22196) is also available for frames and high-touch components.
Isolation Precautions and Zoning in Healthcare Facilities
Transmission-based precautions — contact, droplet, and airborne — require more than PPE and hand hygiene to be effective. Environmental controls are the third leg of the system: room placement, spatial separation, and pathogen-specific surface decontamination protocols must all be implemented together.
Transmission-Based Precautions and Room Protocols
The Joint Commission's 2024 IC.07.01.01 standard introduced Identify-Isolate-Inform (3I) requirements for high-consequence infectious diseases. Compliant programs must include:
- Entry screening for symptoms and travel history
- Documented room placement and isolation procedures
- Notification protocols for public health authorities and key staff
- PPE donning/doffing procedures
- Documented exposure reduction protocols for staff and visitors
CDC supports physical separation of at least 3 feet between beds in multi-patient settings, with privacy curtains drawn between patients during droplet precautions.
Settings without dedicated isolation rooms — open-bay emergency departments, urgent care triage areas, multi-bed recovery bays — present a harder problem. In those environments, portable physical partitioning can create functional separation zones that reduce cross-contamination risk while accommodating care workflows.
Rolascreen's portable retractable screens have been deployed across VA facilities, government health departments, and emergency departments for this purpose. The screens create cleanable spatial separation without construction, extending up to 10'3" wide at standard heights of 5'3" or 6'3".
Special Pathogen Environments
Different pathogens require materially different disinfection approaches:
MRSA and VRE:
- Susceptible to EPA-registered low- and intermediate-level disinfectants at correct dilutions
- VRE can persist on dry surfaces for 7 days to 4 months — pre-cleaning and full contact time are non-negotiable
- CDC monitoring options include direct observation, fluorescent markers, and ATP bioluminescence (cultures not recommended for routine use)
C. difficile:
- Spores can survive on inanimate hospital surfaces for up to 5 months
- Standard hospital disinfectants, including quaternary ammonium products, are not effective against spores
- EPA List K sporicidal products required for terminal cleaning in CDI rooms
- Meticulous pre-cleaning is required first — sporicidal products cannot compensate for uncleaned surfaces
Common Environmental Infection Control Mistakes to Avoid
Most environmental IC failures trace back to a small number of recurring errors:
1. Skipping the cleaning step before disinfection Applying disinfectant to visibly soiled surfaces leaves organic matter that chemically neutralizes the germicide. Incomplete terminal cleaning is both a patient safety failure and a compliance failure — room turnover isn't complete without it. Joint Commission surveyors now verify implementation, not just documentation.
2. Using the wrong disinfectant for the pathogen or surface A quat-based disinfectant in a C. diff-positive room leaves spores viable. A high-level liquid sterilant used on a housekeeping surface creates unnecessary staff exposure risk. The Spaulding Classification and EPA registration system exist specifically to prevent these mismatches — use them.
3. Allowing cleaning equipment to become contamination reservoirs Mop heads left soaking in dirty water, cleaning cloths reused across multiple rooms, bucket solutions not changed after isolation areas — these behaviors transfer rather than remove pathogens. CDC guidance on this is unambiguous: change solutions and replace cloths when visibly soiled and always after isolation room use.
4. Treating porous materials the same as non-porous surfaces Assuming a wipe-down is sufficient for fabric curtains or upholstered furniture is a documented compliance gap. These materials cannot be effectively disinfected with standard hospital products.
Facilities should audit furnishings and partitioning materials for disinfection compatibility as part of their environmental IC program. Any material that cannot support the required disinfection frequency should be replaced with a clinically appropriate alternative — for example, non-porous retractable screens with surfaces compatible with EPA-registered hospital disinfectants, including bleach, quats, and accelerated hydrogen peroxide.

Frequently Asked Questions
What are the current CDC guidelines for infection control?
The CDC's Guidelines for Environmental Infection Control in Health-Care Facilities (originally 2003, updated 2024) is the foundational document, built around six core components:
- Integrate EVS into safety culture
- Train and credential personnel
- Select appropriate cleaning products
- Standardize cleaning protocols
- Monitor adherence
- Provide performance feedback
Who writes the guidelines for environmental infection control in healthcare facilities?
Four bodies govern different compliance areas: the CDC (environmental IC and disinfection), The Joint Commission (accreditation, including the 2024 IC chapter), CMS (Medicare/Medicaid Conditions of Participation), and OSHA (worker safety under 29 CFR 1910.1030). Each targets a distinct layer of compliance — from clinical practice to worker protection.
What are the 5 standards of infection control?
The five standard categories, drawn from CDC Standard Precautions and Transmission-Based Precautions, are:
- Hand hygiene
- Use of personal protective equipment (PPE)
- Cleaning and disinfection of environmental surfaces
- Isolation precautions
- Safe handling of sharps and infectious waste
What is the difference between cleaning, disinfection, and sterilization in healthcare?
Cleaning removes visible dirt and organic matter and is always the required first step. Disinfection uses chemical germicides to inactivate most pathogens and is appropriate for environmental surfaces. Sterilization eliminates all microbial life and is required only for critical instruments that enter sterile tissue.
How often should high-touch surfaces be cleaned in healthcare facilities?
At minimum, daily for occupied patient-care areas — but this is the floor, not the target. Isolation rooms and high-turnover areas require more frequent cleaning, and all high-touch surfaces must be cleaned and disinfected between patients regardless of visible soil.
Are fabric privacy curtains a source of healthcare-associated infections?
Yes. Multiple peer-reviewed studies have found MRSA, VRE, and C. diff on hospital privacy curtains, with contamination occurring within days of laundering. Because porous fabric cannot be wiped with EPA-registered hospital disinfectants, facilities should implement risk-based laundering schedules or replace fabric curtains with non-porous, wipe-clean alternatives — such as retractable privacy screens with medical-grade film panels.