
Key Takeaways
- 1 in 31 hospital patients has an HAI on any given day, costing the U.S. healthcare system up to $33 billion annually
- The five most tracked HAIs—CAUTI, CLABSI, VAP, SSI, and C. diff—are all largely preventable with evidence-based protocols
- Hand hygiene remains the single most cost-effective HAI intervention; each 10% compliance improvement reduces HAIs by 6%
- Environmental surfaces, including high-touch privacy partitions and dividers, are documented pathogen reservoirs that require active management
- CMS penalizes hospitals with the highest HAC scores by 1% of Medicare payments, making infection prevention a financial priority alongside a clinical one
Introduction
According to CDC data, roughly 1 in 31 hospital patients has at least one healthcare-associated infection on any given day. Across U.S. acute-care hospitals, that translates to an estimated 687,000 HAIs annually, with approximately 72,000 deaths among patients who develop them during hospitalization.
The financial toll is equally stark. AHRQ estimates HAIs generate $28 to $33 billion in excess healthcare costs each year—resources consumed treating infections that, in many cases, were preventable.
What makes HAIs especially frustrating for facility leadership is that prevention works. Solutions exist across every layer of care delivery. The gap is consistent, simultaneous implementation across clinical protocols, staff behavior, antibiotic stewardship, and the physical environment patients occupy.
This guide covers:
- The major HAI types and how they spread
- Evidence-based interventions with the strongest track records
- Environmental controls that infection programs frequently overlook
- The regulatory framework holding facilities accountable
What Are Healthcare-Associated Infections?
HAIs are infections patients acquire while receiving treatment for a separate condition. Historically associated with hospitals, the term now applies broadly—urgent care centers, ambulatory surgical centers, nursing facilities, dialysis clinics, and outpatient settings all carry HAI risk.
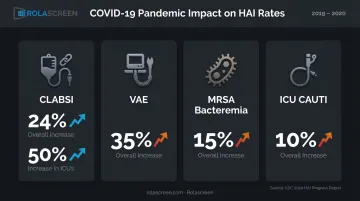
The COVID-19 pandemic exposed how fragile prevention systems can be under surge conditions. The CDC's 2020 HAI Progress Report documented sharp year-over-year increases from 2019 to 2020:
- CLABSI up 24% overall, 50% in ICUs
- VAE (ventilator-associated events) up 35%
- MRSA bacteremia up 15%
- ICU CAUTI up 10%
Recovering from that setback means building prevention systems that hold under surge conditions—not just ones that work when things are calm.
The Five Most Common HAIs and How to Prevent Them
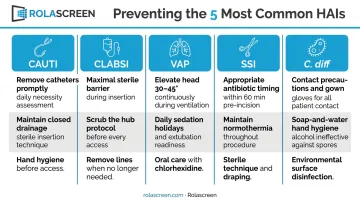
Catheter-Associated Urinary Tract Infections (CAUTI)
Urinary tract infections represent a significant share of nosocomial infections, with the majority tied to indwelling bladder catheters. Duration of catheterization is the primary modifiable risk factor—the longer a catheter remains in place, the higher the infection risk.
Prevention starts with appropriate utilization: use catheters only when clinically indicated and remove them as soon as possible. Insertion technique, sterile supplies, and catheter care protocols all matter, but limiting duration is the foundation.
Central Line–Associated Bloodstream Infections (CLABSI)
Central lines are the leading source of bloodstream HAIs. Key prevention measures include:
- Sterile barrier precautions during insertion
- Chlorhexidine-based skin antisepsis
- Regular line necessity reviews to remove catheters that are no longer clinically required
Modifiable risks — placement technique, catheter type, and duration of use — directly inform each of these interventions.
Ventilator-Associated Pneumonia (VAP)
VAP carries an estimated attributable mortality of around 10%, with higher rates in surgical ICU patients. Prevention focuses on several coordinated interventions:
- Avoiding intubation when alternatives exist
- Minimizing sedation depth and conducting daily extubation readiness assessments
- Maintaining consistent oral hygiene protocols
- Keeping patients positioned appropriately per structured care bundle guidelines
Surgical Site Infections (SSI)
Evidence-based guidelines can prevent up to 60% of SSIs. Key interventions include:
- Surgery-specific antibiotic prophylaxis administered within the correct pre-incision window
- Preoperative patient bathing with antiseptic agents
- Intraoperative skin antisepsis with appropriate agents
- MRSA decolonization screening in high-risk surgical populations
Clostridioides difficile (C. diff)
C. diff is the most commonly reported pathogen in HAI surveillance, and antibiotic exposure is its primary driver. Patients are up to 10 times more likely to develop C. diff while taking antibiotics or within the month after finishing a course.
Core prevention strategies:
- Patient isolation with contact precautions
- Sporicidal environmental cleaning (alcohol-based hand rubs don't kill C. diff spores—soap and water handwashing is required)
- Rigorous antibiotic stewardship to reduce unnecessary exposure
Evidence-Based HAI Prevention Strategies
Hand Hygiene
Hand hygiene is the most consistently recommended and cost-effective single HAI prevention measure. One study cited by CDC found that implementing alcohol-based hand rub systems increased compliance from 38% to 63%—and that each 10% improvement in compliance corresponded to a 6% reduction in overall HAI rates.
Product availability is only the starting point. Structured auditing and real-time feedback programs are what keep compliance rates from drifting—facilities that track hand hygiene behavior consistently outperform those that rely on policy alone.
Personal Protective Equipment (PPE)
PPE protocols differ by transmission route:
| Precaution Type | Applies To | Required PPE |
|---|---|---|
| Standard | All patient contact | Gloves, hand hygiene |
| Contact | MRSA, VRE, C. diff | Gown + gloves |
| Droplet | Influenza, pertussis | Surgical mask |
| Airborne | TB, measles, COVID | N95 + eye protection |
Correct donning and doffing technique is as important as PPE selection—contamination most often occurs during removal.
Antibiotic Stewardship
CDC estimates that approximately 30% of antibiotics prescribed in U.S. acute-care hospitals are unnecessary or suboptimal. That overuse directly fuels C. diff risk and drives antimicrobial resistance across the patient population.
Core stewardship behaviors every facility should standardize:
- Formal antibiotic review at 48–72 hours after initiation
- De-escalation based on culture and sensitivity results
- Documented indication for every antibiotic order at initiation
Vaccination and MDRO Control
Keeping healthcare personnel current on influenza, COVID-19, and other communicable disease vaccines reduces transmission within clinical settings—a direct, if often underemphasized, HAI prevention layer.
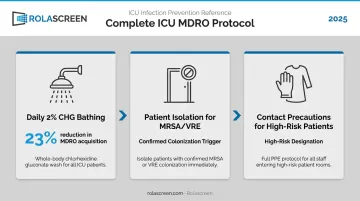
For MDRO control in ICUs, daily 2% chlorhexidine (CHG) bathing cuts transmission rates significantly. A NEJM trial found it reduced overall MDRO acquisition by 23% and hospital-acquired bloodstream infections by 28%.
Paired with CHG bathing, a complete ICU MDRO protocol includes:
- Patient isolation for confirmed MRSA or VRE colonization
- Contact precautions for high-risk individuals
- Consistent CHG application across all ICU patients, not just known carriers
Environmental Controls: The Overlooked Layer of HAI Defense
Clinical protocols get most of the attention in HAI prevention. The physical environment often doesn't, and that gap creates real transmission risk.
Surface Contamination and Prior Room Occupancy
A 2015 systematic review found that patients admitted to rooms previously occupied by infected or colonized patients had 2.14 times higher odds of pathogen acquisition compared to patients admitted to unoccupied rooms. The room itself, not just prior clinical care, carries measurable risk.
This elevates terminal cleaning from a housekeeping function to an infection prevention priority.
Cleaning, Disinfection, and Supplemental Technologies
Routine cleaning manages ongoing contamination between patient interactions. Terminal cleaning—thorough disinfection of every surface after patient discharge or transfer—addresses the accumulated pathogen load.
C. diff and MDRO-contaminated rooms require sporicidal agents, not standard quaternary ammonium products, since quats don't eliminate spores. Increasingly, facilities are supplementing standard cleaning with UV-C light disinfection systems. The BETR cluster-randomized trial found UV-C terminal disinfection reduced target organism acquisition or infection by approximately 30% versus standard cleaning alone—a meaningful additive effect.
The Problem with Fabric Privacy Curtains
Fabric privacy curtains are one of the most consistently overlooked transmission vectors in healthcare settings. A peer-reviewed study published in American Journal of Infection Control found that 41 of 43 sampled curtains (95%) were contaminated at least once, with 21% testing positive for MRSA and 42% for VRE. More telling: 12 of 13 new curtains placed during the study showed contamination within one week.
Fabric is inherently difficult to decontaminate. Its porous structure traps moisture and organisms in a way that wipe-down disinfection can't address—and most facilities lack practical laundering workflows between individual patient uses.
Non-Porous, Wipeable Alternatives
Facilities are replacing fabric curtains with retractable privacy screens featuring non-porous surfaces that can be disinfected with the same EPA-registered hospital disinfectants used on bedrails, IV poles, and equipment. This is precisely what Rolascreen's retractable medical privacy screens are engineered for.
Rolascreen's inner panels are non-porous thermally-stabilized polyester film that resists microbial adhesion and withstands bleach concentrations up to 10,000 ppm — well above the CDC's 5,000 ppm sporicidal threshold for C. diff disinfection. Compatible disinfectants include:
- Sodium hypochlorite (bleach)
- Quaternary ammonium compounds
- Accelerated hydrogen peroxide
Optional silver-ion antimicrobial frame finishes, tested to ISO 22196 standards, address high-touch contact points.
Staff wipe down the screen in the same pass as surrounding surfaces. There's no laundry cycle, no curtain-change workflow, no gap between patients where contaminated fabric hangs in place.

Physical Space Design and Isolation Capacity
The ability to create or reconfigure patient separation zones quickly, without construction, is a genuine infection control capability. In open-bay emergency departments, overflow areas, or any space not designed with individual room isolation in mind, this flexibility matters.
Rolascreen's Portable Elite screens deploy on locking casters, allowing staff to establish separate patient zones rapidly in triage areas, hallways, and temporary care spaces. The screens extend up to 123 inches (10'3") wide, with standard heights of 6'3" and 5'3" and custom heights available. Wall-Mounted Elite and Lite configurations offer a fixed alternative where permanent separation is preferred, with flush or up to 18" extension options.
During COVID-19 surge response, Rolascreen supplied over **200 screens to VA and military facilities** to support rapid patient zone creation—a real-world demonstration of how retractable screen systems can substitute for construction in time-sensitive infection control scenarios. Facilities including Kaiser Permanente, UCSF, and UCLA have integrated these screens into their clinical environments.
Building a Facility-Wide HAI Prevention Program
Institutional Infrastructure
Sustainable HAI reduction requires organizational structure, not just individual-level behavior change. Facilities should establish:
- Infection prevention committees with multidisciplinary representation (nursing, pharmacy, environmental services, administration)
- Standardized care bundles for catheter management, central line insertion, and ventilator care—drawn from CDC STRIVE and SHEA/IDSA guidance
- Ongoing staff education programs tied to surveillance data, not just annual compliance training
CDC's STRIVE infection control training platform (updated 2024) offers modular courses covering both technical and foundational HAI prevention elements at no cost.
Surveillance, Tracking, and Feedback
HAI prevention without measurement is guesswork. CDC's National Healthcare Safety Network (NHSN) is the primary U.S. HAI tracking system, available at no cost to facilities across acute care, long-term care, and outpatient settings.
NHSN enables facilities to:
- Measure infection rates against national benchmarks
- Identify problem areas by unit or care type
- Track progress over time
Sharing surveillance data directly with frontline staff—not just leadership—connects measurement to behavior. Staff who see their own unit's numbers act on them.
Patient and Family Engagement
Patients and families aren't passive participants in HAI prevention. Facilities that actively engage them see measurable benefits. Patients can:
- Speak up when hand hygiene compliance lapses
- Ask whether a catheter or central line is still necessary
- Recognize early signs of infection and report them promptly
- Follow isolation instructions when contact precautions are in place
Education materials, verbal reinforcement from staff, and visible signage all support this engagement—and cost almost nothing to implement.
Regulatory Frameworks and National Standards
HAI prevention carries regulatory weight beyond clinical obligation.
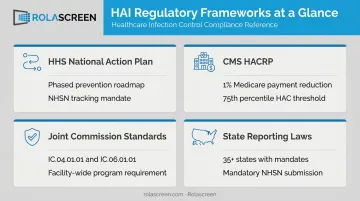
Four overlapping frameworks govern what hospitals must track, report, and improve:
- HHS National Action Plan — A phased prevention roadmap covering acute-care hospitals, ambulatory surgical centers, long-term care facilities, and antibiotic stewardship programs. NHSN tracking and CDC STRIVE training resources are available at no cost.
- CMS HACRP — Applies a 1% Medicare payment reduction to hospitals with Total HAC Scores above the 75th percentile. HAI measures from NHSN feed directly into that scoring methodology, making infection rates a financial variable for CFOs, not just a clinical concern for infection preventionists.
- Joint Commission Standards — Require a facility-wide infection prevention and control program built on active surveillance, prevention, and control activities. Standards IC.04.01.01 and IC.06.01.01 define the structure.
- State Reporting Requirements — More than 35 states have adopted mandatory HAI data submission requirements, most using NHSN reporting. CMS pay-for-performance programs have since expanded those mandates further.
Frequently Asked Questions
What are the most common types of healthcare-associated infections?
The five most widely tracked HAIs are CAUTI, CLABSI, VAP, SSI, and C. diff. All five are considered largely preventable with consistently applied evidence-based protocols across clinical behavior, environmental controls, and antibiotic stewardship.
How does hand hygiene help prevent HAIs?
Hand hygiene breaks the chain of pathogen transmission between patients, surfaces, and healthcare workers. It remains the most consistently recommended single HAI prevention measure—and CDC data shows each 10% improvement in compliance reduces overall HAI rates by approximately 6%.
Are hospital privacy curtains a source of healthcare-associated infections?
Yes. Research has documented that fabric privacy curtains are rapidly colonized with MRSA, VRE, and other pathogens—with new curtains showing contamination within one week of placement. Non-porous, wipeable screen alternatives like Rolascreen's retractable medical privacy screens eliminate this risk by enabling disinfection with standard hospital-grade agents between patient uses.
What is the role of environmental cleaning in HAI prevention?
Routine cleaning reduces ongoing surface contamination; terminal cleaning after patient discharge addresses pathogen reservoirs that accumulate during a stay. High-risk rooms—particularly post-C. diff—require sporicidal agents and may benefit from supplemental UV-C disinfection. Clinical trials show UV-C delivers roughly a 30% additional reduction in target organism acquisition.
What federal standards govern HAI prevention in healthcare facilities?
The HHS HAI National Action Plan sets the strategic framework, with CDC guidelines and NHSN tracking operationalizing it. CMS HACRP ties HAI performance directly to Medicare reimbursement. Joint Commission accreditation standards independently require active facility-wide infection prevention programs.
How can a healthcare facility create patient isolation zones without major construction?
Portable retractable privacy screens can be rapidly deployed in open-bay areas, hallways, and overflow spaces to create physical separation between patients. Systems like Rolascreen's Portable Elite screens support contact and droplet precaution protocols without structural renovation, deploying on locking casters and extending up to 10'3" wide to accommodate varied space configurations.


