Introduction
Schools are among the most challenging environments to keep infection-free. Hundreds of students packed into classrooms for six to eight hours daily, sharing desks, devices, water fountains, and doorknobs — it creates ideal conditions for pathogens to move quickly through a population.
The consequences aren't abstract. According to CDC's National Survey of Children's Health, more than two-thirds of children missed at least one school day due to illness or injury in 2022. When outbreaks hit, absenteeism spikes, staff shortages follow, and learning continuity breaks down.
This guide is written for school administrators, health staff, and facility managers who need more than hand-washing posters. It covers:
- Why schools are structurally high-risk environments
- The four main transmission routes in school settings
- A layered prevention framework and environmental controls
- Isolation protocols and how to build a school IPC plan that works in practice
Key Takeaways
- Schools face elevated infection risk due to crowding, long contact times, shared surfaces, and inconsistent hygiene habits in younger students
- A layered "Swiss Cheese" approach combining hygiene, ventilation, disinfection, vaccination, and physical barriers provides the strongest protection
- Standard precautions apply across every shared school space — classrooms, cafeterias, restrooms, and hallways alike
- Designated isolation areas for symptomatic students are underutilized but highly effective
- A written IPC plan with defined outbreak thresholds is essential for maintaining school operations during outbreaks
Why Schools Are High-Risk Environments for Infectious Disease
The Structural Problem
No matter how well a school is managed, its basic design works against infection control. Students spend hours in close proximity every day — a contact-network study of Utah middle schoolers found they averaged 338 to 348 minutes of daily contact time. Elementary students averaged 257 to 305 minutes. That's sustained, repeated exposure across hundreds of peers.
Younger children compound the problem. Handwashing compliance is inconsistent, cough etiquette is rarely instinctive, and many children haven't yet built immunity to common pathogens. Objects get shared without a second thought: pencils, tablets, sports equipment, playground fixtures.
Common Infections in School Settings
The diseases that circulate most frequently in K-12 environments include:
- Influenza — spreads via droplets and contact; causes significant seasonal absenteeism
- Norovirus — highly contagious; spreads through contact and fecal-oral routes
- Strep throat — droplet and contact transmission; clusters easily in classrooms
- RSV — particularly serious for younger and immunocompromised students
- Common cold viruses — airborne and contact; endemic in school populations
- COVID-19 — airborne, droplet, and contact transmission; variable severity
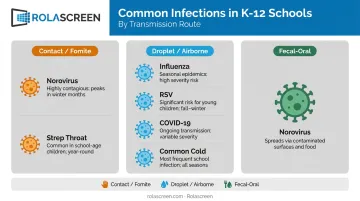
Each pathogen follows a different primary transmission route. That's why a single-measure approach to infection prevention consistently falls short in school settings.
How Infections Spread in School Settings
Schools are high-density environments where pathogens move through multiple routes simultaneously — knowing which ones dominate shapes every IPC decision.
Contact and Fomite Transmission
Direct contact — handshakes, touching a sick peer — is one pathway. More prevalent in schools is indirect contact via fomites: contaminated surfaces that transfer pathogens to hands, then to mucous membranes.
A study of six Washington elementary school classrooms found influenza A on up to 50% of sampled surfaces and norovirus on up to 22%. The most frequently contaminated objects were:
- Water fountain toggles and faucet handles
- Pencil sharpeners and keyboards
- Desktops and shared classroom surfaces
These are surfaces students touch dozens of times per day.
Droplet and Airborne Transmission
When someone coughs or sneezes, large respiratory droplets containing pathogens can travel approximately six feet — enough to reach adjacent desks in a standard classroom arrangement. Influenza, strep, and RSV spread primarily this way.
Airborne transmission involves smaller aerosol particles that can linger and travel beyond six feet, particularly in poorly ventilated spaces. This matters most for COVID-19 and measles, and it's why ventilation is a genuine IPC lever, not just a comfort issue.
Fecal-Oral and Other Routes
For younger students especially, the fecal-oral route creates real exposure risk. Diapering, toileting assistance, cafeteria food handling, and classroom pets are all potential vectors. Hand hygiene — consistent, technique-correct handwashing — is the primary control.
In the school health office specifically, bloodborne transmission risk exists wherever sharps are used. Standard precautions, the same baseline used in clinical settings, apply here without exception.
The Layered Approach to Infection Prevention in Schools
No single measure eliminates infection risk. The "Swiss Cheese" model of IPC stacks multiple overlapping strategies, each with different strengths, so that where one has gaps another compensates. CDC's consolidated K-12 guidance is built on this principle.
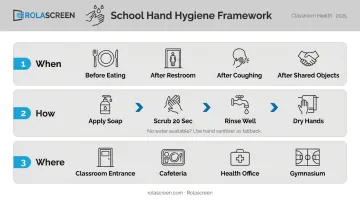
Hand Hygiene
Hands are the most common pathway for germ transmission — and hand hygiene is the most reliable way to interrupt it. CDC data shows that handwashing education in communities reduces absenteeism due to gastrointestinal illness in schoolchildren by 29% to 57%.
Practical implementation in schools:
- When: Before eating, after using the restroom, after coughing/sneezing, after handling shared objects
- How: Soap and water for at least 20 seconds; alcohol-based sanitizer (minimum 60% alcohol) when soap isn't available
- Where: Place sanitizer stations at classroom entrances, cafeteria entry points, health office waiting areas, and gymnasium entrances
- Modeling: Staff behavior matters — students follow what they see adults do
Respiratory Hygiene and Cough Etiquette
Core practices to reinforce school-wide:
- Cover coughs and sneezes with a tissue or elbow, not hands
- Provide no-touch disposal bins at eye level near high-traffic areas
- During elevated transmission periods, encourage mask use among symptomatic individuals in high-risk settings
- Post clear stay-home guidance for families — symptomatic students expose dozens of peers before anyone realizes they're contagious
Proactive family communication reduces the volume of infectious individuals in the building before symptoms escalate.
Vaccination
Vaccination reduces the size of the susceptible population, which limits how far an outbreak can spread. School-entry requirements exist for this reason — state and local vaccination requirements are recognized by CDC as important tools for maintaining high coverage rates.
Coverage gaps matter. CDC's 2023–24 kindergarten data found the exemption rate reached 3.3% nationally, with exemptions exceeding 5% in 14 jurisdictions — thresholds that create meaningful outbreak vulnerability.
School-based vaccination clinics improve access and uptake, particularly for annual flu vaccines. A school-located influenza vaccination study found influenza rates were 27.1 vs. 60.0 per 1,000 children in vaccinated vs. control schools, with unvaccinated children missing more school days as well.
Cleaning, Sanitizing, and Disinfecting
These three terms have distinct meanings:
| Term | What It Does |
|---|---|
| Cleaning | Physically removes dirt and reduces germ load using soap and water |
| Sanitizing | Reduces remaining germs after cleaning to safe levels |
| Disinfecting | Uses chemicals to kill harmful germs on already-cleaned surfaces |
All three steps matter, and the sequence matters. Disinfecting a dirty surface is far less effective than cleaning first. For schools, daily disinfection of high-touch surfaces — desktops, doorknobs, light switches, restroom fixtures, shared devices — using EPA-registered products should be standard practice.
The same Washington elementary school study found that daily quaternary ammonium disinfection wipes were associated with lower surface contamination, and control-group students were 2.32 times more likely to experience absenteeism than students in intervention classrooms.
Custodial staff training on proper product use, dwell times, and surface coverage directly determines whether disinfection actually works. Without it, even the right products deliver inconsistent results.
Environmental Controls: Ventilation, Physical Space, and Barriers
Indoor Air Quality
Ventilation is an underutilized IPC tool. A Georgia MMWR study found COVID-19 incidence was 39% lower in schools that improved ventilation; combining dilution and filtration strategies was associated with 48% lower incidence.
The infrastructure gap is significant: NCES data shows 30% of public schools with permanent buildings rated their HVAC or ventilation systems as fair or poor. Among portable buildings, that figure rises to 41%.
Practical ventilation strategies schools can act on now:
- Open windows and doors when weather and security allow
- Inspect and validate HVAC systems annually; replace filters on schedule
- Deploy portable HEPA air purifiers in classrooms and health offices (28% of surveyed K-12 schools already use them)
- Use CO₂ monitors to identify poorly ventilated spaces — readings consistently above 1,000 ppm suggest inadequate fresh air exchange

Designated Isolation Areas
CDC guidance recommends that schools proactively identify spaces to separate sick students from healthy peers while they wait for pickup. The ideal isolation space allows staff monitoring, has a separating door, and has increased air circulation.
This matters because the typical school health office waiting area becomes a concentration point for symptomatic students — mixing them with students who need routine care or minor first aid creates unnecessary exposure.
Physical Barriers for Rapid Space Reconfiguration
Many schools can't dedicate a separate room exclusively to isolation. The practical alternative: portable, retractable privacy screens that create a physical barrier between symptomatic and healthy students without construction or permanent modification.
Rolascreen's retractable privacy screens are built for exactly this use case. Their panels use non-porous thermally-stabilized polyester film, wipeable with EPA-registered hospital disinfectants — bleach solutions, quaternary ammonium compounds, and accelerated hydrogen peroxide.
The retractable design means an isolation zone can be activated during an outbreak and returned to normal use within minutes — no construction, no permanent room loss.
Two configurations suit different school environments:
- Portable Elite (wheeled) — flexible deployment across rooms without wall modifications, ideal for variable day-to-day needs
- Wall-Mounted Elite — a fixed solution for health offices where isolation capacity is needed consistently
Material choice matters here. Fabric curtains — common in health office bay configurations — are porous and harbor pathogens. Any partition used in an IPC context must be made of a cleanable, non-porous material to avoid harboring and transferring pathogens. Damaged or soiled fabric dividers should be replaced, not cleaned.
Waste Management in the Health Office
Standard environmental controls in the health office also include:
- Sharps containers in any area where needles are used
- No-touch tissue disposal bins throughout the health office and isolation area
- Regular waste removal — don't let high-risk waste accumulate between custodial rounds
Managing Sick Students and Staff: Isolation and Exclusion
When to Stay Home
CDC guidance is specific about exclusion triggers. Students and staff should stay home when they have:
- Fever (with or without rash)
- Vomiting more than twice in 24 hours
- Diarrhea causing accidents, or more than 2 stools above normal in 24 hours
- Draining skin sores that cannot be covered
- Worsening respiratory symptoms
Return is appropriate after 24 hours fever-free without fever-reducing medication, with vomiting or diarrhea resolved, and respiratory symptoms improving for at least 24 hours. These thresholds should be written into school policy and communicated clearly to families before illness season.
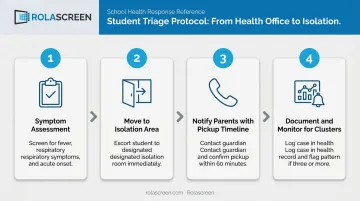
Triage and Isolation While Awaiting Pickup
The school nurse's role during elevated illness periods includes:
- Assessing symptoms when students arrive at the health office
- Moving symptomatic students to a designated isolation area, separated from healthy students waiting for routine care
- Notifying parents promptly with clear pickup expectations
- Documenting each case — clusters of similar presentations in the same grade or classroom are early outbreak signals
Communication with Families
Schools should communicate illness thresholds and return-to-school criteria proactively — not just when an outbreak is already happening. Practical steps that make a measurable difference:
- Send exclusion criteria and return thresholds home in back-to-school packets before illness season
- Provide multilingual versions so all families can act on the information
- Use the school app or email to push reminders at the start of flu season
- Train front office staff to reference written policy when parents call to dispute exclusions
Building a School IPC Plan: From Policy to Practice
What the Plan Should Include
A functional school IPC plan isn't a separate document — it lives within the school's Emergency Operations Plan (EOP) as a dedicated infectious disease section. Core components:
- Defined roles and responsibilities — who decides to activate outbreak protocols, who contacts local public health, who manages family communication
- Outbreak thresholds — specific criteria that trigger escalating responses (e.g., 10% absenteeism in a single classroom, confirmed lab-positive norovirus case)
- Communication protocols with local health departments, established before an outbreak
- Supply inventory — hand sanitizer, PPE, EPA-approved disinfectants, tissues, physical barriers — maintained year-round, not restocked reactively
Staff Training
All school staff — not just health personnel — need annual, role-specific training covering:
- Hand hygiene and respiratory etiquette
- What to do when a student appears symptomatic in class
- PPE use in applicable situations (health office staff, those providing first aid)
- Cleaning protocols for shared spaces
A school nurse following perfect protocol can't compensate for a teacher who sends symptomatic students to the water fountain and back. Every staff member's behavior either reinforces or undermines the layers above it.
Annual Review
IPC plans should be reviewed annually, ideally with input from local public health partners. Review timing: late summer, before school starts. Each review should address:
- Prior year's absenteeism trends and documented illness clusters
- Any outbreak responses — what worked, what didn't
- Protocol gaps identified during the year
- Supply inventory confirmation before flu season begins
Frequently Asked Questions
What precautions can you take in school to reduce infectious diseases?
The highest-impact everyday actions are frequent handwashing with soap and water, respiratory hygiene (covering coughs and sneezes), daily disinfection of high-touch surfaces, improving classroom ventilation, staying current on vaccinations, and enforcing clear stay-home policies for symptomatic students and staff.
What are the 5 standard precautions for infection control?
In school health office settings, standard precautions include: proper hand and respiratory hygiene, appropriate use of personal protective equipment (gloves, masks where indicated), cleaning and disinfection of environmental surfaces, safe handling and disposal of sharps, and proper handling of potentially contaminated materials. These apply in school health offices just as they do in clinical settings.
What are the 5 F's of infection control?
The 5 F's — Fingers, Food, Flies, Feces, and Fomites — describe common pathways for fecal-oral pathogen transmission. In schools, all five are relevant: unwashed hands (fingers), cafeteria food handling (food), outdoor environments (flies), toileting assistance with younger students (feces), and contaminated shared surfaces (fomites).
Why are schools considered high-risk environments for infectious disease outbreaks?
High-density crowding, long daily contact times (6–8 hours), inconsistent hygiene habits among children, dozens of shared surfaces, and the presence of younger students with limited prior immunity all combine to create elevated transmission risk. Contact tracing studies show elementary students average over 300 daily interactions with peers.
How should schools isolate sick students while waiting for pickup?
Symptomatic students should be moved immediately to a designated isolation area physically separated from the main health office waiting area — either a separate room or a partitioned space. The isolation area should allow staff monitoring and have adequate air circulation. Using portable retractable barriers can create this separation in health offices without a dedicated room.
When should a student be allowed to return to school after illness?
General CDC guidance supports return after 24 hours fever-free without fever-reducing medication, with vomiting and diarrhea resolved. For diseases like norovirus, influenza, or strep throat, consult CDC disease-specific guidance and local public health requirements — some conditions require longer exclusion periods or a negative test before return.