Antimicrobial finishes are one layer of that defense. This guide explains what they are, how they work, where they matter most in clinical settings, and what procurement teams should look for when evaluating products.
Key Takeaways
- Antimicrobial finishes inhibit or destroy microorganisms on treated surfaces — they supplement cleaning, they don't replace it
- Common types include silver ion, QACs, N-halamines, zinc oxide, and chitosan — each with distinct mechanisms and durability profiles
- Highest-priority healthcare applications include privacy screens, cubicle curtains, upholstery, and patient room surfaces
- Always request third-party test data against standards like AATCC 100, ISO 20743, or ASTM E2149 before specifying a product
- Non-porous, wipeable surfaces like Rolascreen's retractable privacy screens offer a structurally different approach to infection control than treated fabrics
What Is an Antimicrobial Finish?
An antimicrobial finish is a chemical treatment applied to a surface, fabric, or material that inhibits the growth, reproduction, or survival of microorganisms — including bacteria, fungi, mold, and in some formulations, certain viruses.
The EPA defines antimicrobial pesticides as substances used to destroy or suppress harmful microorganisms on inanimate objects and surfaces.
Antimicrobial vs. Antibacterial vs. Antiviral
These terms are not interchangeable, and products are frequently mislabeled:
- Antimicrobial — broad-spectrum; targets bacteria, fungi, mold, and sometimes viruses
- Antibacterial — bacteria-specific; does not address fungi or viruses
- Antiviral — virus-specific; does not cover bacterial contamination
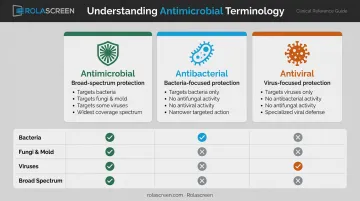
For healthcare procurement, understanding this distinction has direct clinical consequences. A curtain treated with an antibacterial finish offers no protection against Candida auris or norovirus. Specifying the wrong product for the environment is a common and avoidable mistake.
Where Finishes Are Applied
Antimicrobial treatments can be applied to virtually any material or surface:
- Textiles and fabrics — cubicle curtains, upholstery, exam table covers, gowns
- Hard surfaces — partitions, wall panels, room dividers
- Coatings — paint, vinyl films, surface sprays
- Impregnated during manufacturing — the agent is embedded in the polymer matrix before the product is formed, offering longer-lasting protection than surface-applied treatments
A Critical Limitation
An antimicrobial finish does not sterilize a surface. Its effectiveness depends on several factors:
- The specific microorganism type being targeted
- The chemistry and age of the finish
- The cleaning practices used alongside it
Antimicrobial finishes do not eliminate established biofilm on their own. Facilities that treat them as a substitute for cleaning protocols — rather than a complement — will see diminishing returns.
How Antimicrobial Finishes Work: Mechanisms and Types
At a cellular level, antimicrobial agents attack microorganisms through several pathways: disrupting cell membranes, inhibiting enzyme function, generating oxidative stress, or interfering with DNA replication. The chemistry used determines which pathway dominates — and how durable that protection is in real-world use.
Metallic Compounds: Silver Ion, Zinc Oxide, Titanium Dioxide
Silver ion (Ag+) is one of the most researched antimicrobial agents in clinical use. When silver oxidizes on contact with moisture, it releases Ag+ ions that work through multiple simultaneous pathways:
- Disrupts bacterial cell membranes on contact
- Binds to thiol groups in enzymes, impairing metabolic function
- Inhibits respiratory chains
- Interacts directly with DNA
A 2021 peer-reviewed review confirms broad activity against both gram-positive and gram-negative bacteria through these combined mechanisms.
One important caveat: the same research shows that repeated sublethal silver exposure can increase minimum inhibitory concentrations (the dose required to stop bacterial growth) in organisms like E. coli and S. aureus. Silver's efficacy is well-documented, but resistance potential isn't zero. At effective concentrations in approved formulations, silver is considered generally safe for human contact — though cytotoxicity can be dose-dependent and influenced by particle size and coating.
Zinc oxide is a cost-effective alternative with additional UV-blocking properties, well-suited for textiles and coatings in bright or outdoor-adjacent environments. Titanium dioxide acts as a photocatalyst — it requires UV light activation to generate the reactive oxygen species that damage microbial membranes, making it most effective in spaces with consistent light exposure rather than enclosed or dim clinical settings.
Not all metallic agents are interchangeable. Matching the chemistry to the environment is what determines performance.
Quaternary Ammonium Compounds (QACs)
Where metallic agents rely on ionic chemistry, QACs take a physical approach: the positively charged head group binds to negatively charged microbial surfaces, while hydrophobic chains penetrate and destabilize the lipid cell membrane. They're effective against gram-positive and gram-negative bacteria, fungi, and some viruses.
The concern with QACs in prolonged use is tolerance development. A 2023 review identified mechanisms including efflux pumps, membrane changes, and biofilm formation that allow some organisms to survive repeated QAC exposure. That same review documented 43 episodes of contaminated in-use QAC disinfectants in hospitals, including 26 infection outbreaks — a relevant risk for facilities using QAC-treated surfaces alongside QAC-based cleaning agents.
N-Halamines
N-halamines form oxidative N-Cl bonds that transfer active chlorine to microbial cells, causing broad-spectrum oxidative damage. Their practical advantage in textile applications: when the biocidal chlorine is depleted, N-halamine finishes can be recharged by laundering with bleach, restoring antimicrobial activity. This makes them a strong option for reusable clinical textiles with predictable laundry cycles.
Natural and Emerging Agents
Chitosan (derived from shellfish chitin) and plant-based extracts like neem offer biodegradable, lower-toxicity alternatives with genuine antimicrobial activity. Nano-material-based finishes are an active area of development, but regulatory clarity — particularly from the EPA — is still evolving for many formulations.
Where Antimicrobial Finishes Are Used in Healthcare
AHRQ data shows more than 1 million HAIs occur across the U.S. healthcare system every year, costing billions in direct medical expenses. Reducing pathogen load on high-contact surfaces is one of the few interventions that can be applied across an entire facility simultaneously.
High-Touch Textile Surfaces
Fabric surfaces see the most frequent patient and staff contact — and are the hardest to keep clean. Key applications include:
- Patient room upholstery and recliners
- Cubicle curtains and privacy curtains
- Exam table covers
- Behavioral health and dialysis seating
- Waiting room furniture
A 2023 study found that standard privacy curtains carried an average of 32.6 CFU of bacterial contamination, compared to 0.56 CFU on antimicrobial and sporicidal replacement curtains — a dramatic difference driven purely by surface treatment. Hospital curtains are high-touch, cleaned infrequently, and documented as pathogen reservoirs between laundry cycles.
Hard Surfaces, Partitions, and Privacy Screens
Antimicrobial protection on hard surfaces operates differently. The goal isn't just treating the material — it's selecting surfaces that can be disinfected thoroughly and repeatedly without degrading.
Non-porous, wipeable surfaces have a structural advantage over fabric: pathogens can't be mechanically trapped in a fiber matrix they can't penetrate. For privacy screens and room dividers, that distinction matters considerably.
Rolascreen's retractable privacy screens use a thermally-stabilized medical-grade polyester film that resists microbial adhesion through surface tension rather than physical trapping. The panels withstand bleach concentrations up to 10,000 ppm — above the CDC's 5,000 ppm sporicidal threshold required for C. difficile contact-precaution rooms.

Rolascreen also offers an optional antimicrobial finish service applied to these non-porous panels for infection-control-sensitive environments. For facilities evaluating total infection control strategy in open-bay areas, emergency departments, or multi-patient rooms, the combination of non-porous construction and optional antimicrobial treatment is worth evaluating alongside fabric alternatives.
Beyond Healthcare
Antimicrobial finishes appear across several other industries:
- Sportswear fabrics treated to inhibit odor-causing bacteria in moisture-wicking materials
- Hospitality bedding and upholstery in high-turnover hotel and resort environments
- Food processing equipment and workstation surfaces to limit cross-contamination
- PPE including masks, gowns, and gloves for an added barrier layer
Outside healthcare, performance and durability requirements vary widely — which is exactly why the clinical environment demands a higher bar for testing, documentation, and verified efficacy.
What to Look for When Evaluating Antimicrobial Surfaces and Finishes
Documented Efficacy Testing
Marketing language is not evidence. Look for products tested against recognized standards:
| Standard | Type | Application |
|---|---|---|
| AATCC 100 | Quantitative antibacterial | Textile materials |
| AATCC 147 | Qualitative (parallel streak) | Textile screening |
| ISO 20743 | Quantitative antibacterial | Textiles including nonwovens, bedding |
| ASTM E2149 | Dynamic contact conditions | Antimicrobial-treated specimens |
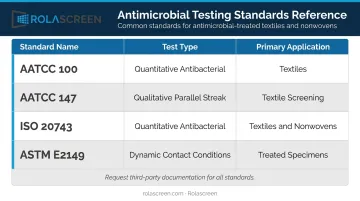
Request third-party test documentation. In-house claims from manufacturers without independent verification are not sufficient for healthcare procurement.
Compatibility with Cleaning Protocols
Once you've confirmed test data, verify the finish holds up to real-world cleaning. It must survive the disinfectants actually used in your facility without losing efficacy or degrading the substrate:
- Bleach solutions
- Quaternary ammonium compounds (QACs)
- Accelerated hydrogen peroxide
For hard surfaces and privacy screens, non-porous construction is critical — it supports complete wipe-down disinfection without fluid absorption.
Substrate Suitability
Chemistry that performs on polyester fabric may not translate to vinyl, coated hard panels, or non-porous film. Confirm the finish is appropriate for the actual surface type, and verify it doesn't compromise functional properties such as color stability, structural integrity, or cleanability under your protocols.
Antimicrobial Finishes vs. Routine Cleaning
Antimicrobial finishes reduce microbial load between cleaning events. They slow recolonization after disinfection, extending the effective hygiene window during high-traffic periods when cleaning can't happen immediately. That's a genuine benefit — but it's not a substitute for scheduled disinfection.
The practical model looks like this:
- Physical barriers — partitions, screens, and room dividers create spatial separation and reduce cross-contamination pathways
- Surface treatments — antimicrobial finishes slow microbial recolonization on treated materials
- Cleaning protocols — scheduled disinfection removes established contamination and biofilm
- Hand hygiene — the single most evidence-supported HAI prevention measure
Each layer addresses what the others can't. Copper-oxide composite surfaces in a 2016 study were associated with a 78% reduction in MDRO and C. difficile HAIs when used alongside standard cleaning protocols — a result that holds only when surface treatments complement, not replace, scheduled disinfection.

That combination matters. Facilities that lean on antimicrobial finishes as a standalone solution will eventually see those benefits erode — the finish is one layer in a hierarchy of controls, and its value depends on the layers around it.
Frequently Asked Questions
What is the difference between antimicrobial and antibacterial finishes?
Antibacterial finishes target bacteria only. Antimicrobial finishes cover a broader spectrum — bacteria, fungi, mold, and in some formulations, certain viruses. For most clinical environments, antimicrobial is the appropriate specification; antibacterial alone may leave gaps in protection against fungal pathogens like Candida auris.
Is antimicrobial coating safe?
Most commercially approved coatings — including silver ion and QAC-based treatments — are considered safe at effective concentrations and are regulated by the EPA under FIFRA. Look for an EPA registration number on the product label and request a Safety Data Sheet (SDS) from any supplier before specifying for clinical use.
How long does an antimicrobial finish last?
Durability varies by type: finishes incorporated during manufacturing typically last the product's useful life, while surface-applied treatments may degrade with repeated cleaning. Always ask suppliers for cleaning-cycle durability data before committing to a specification.
Does an antimicrobial finish replace regular cleaning in healthcare settings?
No. Antimicrobial finishes reduce microbial load between cleaning events and slow recolonization, but they don't sterilize surfaces or eliminate established biofilm. Standard disinfection protocols remain mandatory for regulatory compliance and effective infection control.
What are examples of antimicrobial coatings?
Common examples include silver ion coatings, QAC treatments, zinc oxide nanoparticle coatings, N-halamine finishes, titanium dioxide photocatalytic coatings, and chitosan-based natural coatings. Each is suited to specific substrates, environments, and activity spectrums.
Are antimicrobial finishes tested to recognized standards?
Yes. Recognized standards include AATCC 100, AATCC 147, ISO 20743, and ASTM E2149. For clinical procurement, always request documentation of third-party testing against at least one of these standards before specifying a product for patient care environments.