Introduction
Dialysis patients are immunocompromised by definition. They spend 3 to 4 hours per session, three times a week, in close proximity to shared bay partitions — surfaces that accumulate touch, aerosol, and organic residue across multiple patient encounters. CDC NHSN data reported 14,822 bloodstream infections in 2020 dialysis-facility surveillance, with Staphylococcus aureus accounting for 34.2% of those infections and MRSA comprising nearly 38% of S. aureus isolates.
Standard cleaning addresses what's visible. It does not address what persists between sessions on high-contact partition surfaces.
This guide is written for dialysis center managers, infection control coordinators, and facilities teams responsible for implementing antimicrobial coatings on bay partitions.
Getting these coatings right requires compatible surfaces, proper preparation, and a validated application sequence. Skip steps and you get coating failure, premature degradation, or false compliance confidence. This guide covers all of it: surface assessment, step-by-step application, post-application validation, and the most common problems facilities encounter.
Key Takeaways
- Dialysis bay partitions are high-touch surfaces that standard session cleaning alone cannot fully protect.
- Surface preparation — not the coating itself — is the most common cause of premature coating failure.
- Non-porous, wipeable panel surfaces hold antimicrobial coatings far better than porous or fabric-based alternatives.
- Coatings complement regular disinfection protocols; they do not replace them.
- Plan reapplication intervals more frequently than manufacturer defaults — dialysis environments see heavy alcohol and disinfectant wipe use.
Prerequisites and Preparation for Coating Dialysis Bay Partitions
Surface preparation determines coating performance more than any other factor. A coating applied to a contaminated, chemically incompatible, or structurally degraded surface will fail prematurely or deliver only partial coverage — which is worse than no coating at all, because it creates false confidence.
Surface and Material Compatibility
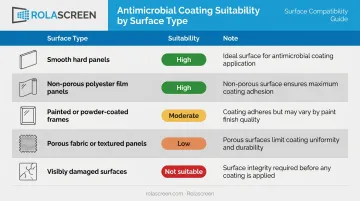
Not all partition surfaces accept antimicrobial coatings equally. The table below summarizes what facilities typically encounter:
| Surface Type | Coating Suitability | Notes |
|---|---|---|
| Smooth hard panels (coated PVC, acrylic) | High | Strong adhesion, meets EPA/ISO non-porous testing scope |
| Non-porous polyester film panels | High | Ideal — wipeable, chemically resistant, no fiber matrix |
| Painted or powder-coated frames | Moderate | Confirm coating chemistry compatibility first |
| Porous fabric curtains or textured panels | Low | Uneven absorption, inconsistent coverage, different test standards apply |
| Visibly damaged or degraded surfaces | Not suitable | Repair or replace before any coating application |
EPA guidance on residual antimicrobial products applies to hard, non-porous, non-food-contact surfaces, and ISO 22196 — the primary standard for measuring antibacterial activity — addresses non-porous materials specifically. Porous and textile surfaces require entirely different test protocols (ISO 20743, ISO 18184), which means antimicrobial performance claims are not transferable from one surface category to another.
That surface category distinction is why partition material selection matters before coating ever begins. Rolascreen's retractable privacy screens use non-porous thermally stabilized medical-grade polyester film panels validated for compatibility with bleach (up to 10,000 ppm), quaternary ammonium compounds, and accelerated hydrogen peroxide. That inherent chemical resistance makes them compatible with a broader range of coating chemistries and reduces the risk of surface-coating interaction problems.
Non-negotiable rule: If a partition surface is visibly damaged, degraded, or made from a porous material that cannot meet clinical cleaning standards, do not apply coating. Address the surface first.
Cleaning and Surface Readiness
Before coating, the surface must be free of:
- Biofilm (dry biofilms on healthcare surfaces can reduce disinfectant susceptibility and interfere with coating adhesion)
- Residual disinfectant — particularly alcohol-based or quaternary ammonium wipes
- Particulates and organic debris
Tools and materials needed:
| Item | Essential or Optional |
|---|---|
| Compatible neutral cleaner (per coating manufacturer's spec) | Essential |
| Lint-free application cloths or spray applicator | Essential |
| PPE: gloves, mask | Essential |
| Manufacturer-required primer or activator | Essential if specified |
| Directional light source for visual inspection | Recommended |
Facilities often overlook one step: allow full drying after the pre-application clean before coating. EPA moisture guidance confirms that residual moisture or chemical residue can adversely affect coating durability. The exact required dry interval is label-specific — check your coating product, not a generic guideline.
Step-by-Step: How to Apply Antimicrobial Coating to Dialysis Bay Partitions
The application sequence matters. Cutting steps or rushing dwell times are the most consistent causes of underperforming coatings in real clinical environments.
Preparing the Application Environment
Before touching the coating:
- Fully extend the partition — retractable screens must be completely deployed. Applying to a partially extended screen leaves overlapping sections untreated.
- Ensure ventilation — solvent-based coatings require air exchange. Open windows or activate HVAC where possible.
- Clear patient materials and equipment from the bay — coating overspray on medical equipment or patient chairs creates unnecessary complications.
- Confirm the surface is dry — visually and by touch. Do not proceed if the surface feels cool or damp from a recent wipe-down.
Applying the Coating
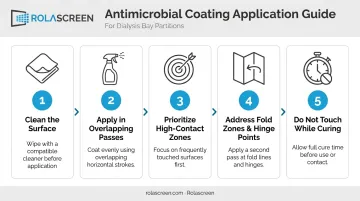
Follow the manufacturer's recommended application method (spray, wipe, or brush). The process generally follows this sequence:
- Wipe down the full surface with the manufacturer's specified compatible cleaner — not a general disinfectant.
- Apply coating in even, overlapping passes — no pooling, no missed zones.
- Prioritize high-contact zones: edges, lower panels, handles, and any frame components.
- Address fold zones and hinge points specifically — on retractable partitions, these areas are frequently missed. Apply a second thin pass over all fold transition points.
- Do not touch the surface during curing — observe the full drying time per manufacturer instructions.
Uneven application is not a minor cosmetic issue. It creates gaps in antimicrobial coverage that are invisible to the eye but detectable through post-application microbiological testing. A uniform sheen or texture across the entire surface is the goal.
For retractable screens specifically, the coating must cover the full extended surface — not just the face visible when the screen is partially deployed. Handles and mechanical contact points are high-touch by definition; treat them as priority zones, not afterthoughts.
Integrating Coating into the Cleaning Schedule
Timing the coating application correctly makes a measurable difference:
- Apply after a full terminal clean — not after a quick between-session wipe-down.
- Allow the surface to dry completely before coating. Applying immediately after a disinfectant wipe-down — even if the surface looks dry — risks adhesion failure from residual chemistry.
- Schedule during shift downtime, not between individual patient sessions. Most coatings require a curing window that cannot be compressed without sacrificing performance.
On reapplication frequency: a 2023 study of a QAC-based coating on PVC, glass, and stainless steel found antimicrobial activity lasted less than one week under standard cleaning conditions, despite longer manufacturer claims. In dialysis settings — where station surfaces are disinfected after every patient per APIC and CDC protocols — most coatings degrade faster than general manufacturer intervals anticipate.
Verify reapplication timing directly with your coating manufacturer based on the specific cleaning agents and session volumes in your facility.
Post-Application Checks and Validation
Returning a partition to patient use without confirming successful coating application is a risk that is easy to avoid and hard to justify during an audit.
Visual and Functional Checks
A proper visual check takes two to three minutes and should confirm:
- No streaking, pooling, or missed zones across the full panel surface
- Uniform sheen or texture consistent with what the manufacturer describes for a correctly applied coat
- No lifting, bubbling, or adhesive separation on smooth panel surfaces
- Full coverage at fold points, edges, and handles — use directional light to inspect these areas, as many coatings are colorless and nearly invisible under standard lighting
Document the check. Record the date, the technician who performed the application, the coating product and lot number, and the next scheduled reapplication date.
This documentation directly supports APIC and CMS compliance requirements. 42 CFR 494.30 requires dialysis facilities to provide and monitor a sanitary environment to minimize infectious agent transmission, and CMS interpretive guidance expects surface disinfection records to be maintained with specificity. An auditor reviewing incomplete or missing validation records will flag it as a compliance gap.
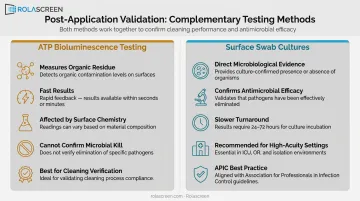
Microbiological Spot-Check (Optional but Recommended)
For facilities trialing a new coating product or coating for the first time, ATP bioluminescence testing provides a measurable baseline. It measures organic residue on the surface and can confirm cleaning quality before and after application.
Keep its limitations in mind before drawing conclusions:
- ATP measures adenosine triphosphate — an organic material marker — not microbial kill specifically
- Readings can be affected by surface characteristics and disinfectant residues
- ATP cannot distinguish microbial from non-microbial organic material
Use it as a cleaning-verification tool, not as proof of antimicrobial coating efficacy. Where more direct confirmation is needed, surface swab cultures offer microbiological evidence ATP cannot. In high-acuity dialysis settings, APIC and infection control teams treat this level of post-application verification as best practice.
Common Coating Application Problems and Fixes
Coating Delaminating or Peeling After Cleaning
What you'll see: Visible lifting, flaking, or wear patterns appearing within days of application.
Why it happens:
- Residual disinfectant or alcohol present on the surface at time of application
- Incompatible surface material
- Insufficient drying time between cleaning and coating
Fix: Strip the affected area, allow full drying (confirm per manufacturer guidance), re-clean with a compatible neutral cleaner, and reapply following the manufacturer's dwell time requirements exactly.
Uneven Coverage Across Retractable Panels
What you'll see: Post-application testing shows higher contamination in specific zones; the antimicrobial effect is inconsistent across the surface.
Why it happens:
- Coating applied while the screen was partially retracted, leaving folded-over sections untreated
- Pooling at fold transition points
Fix: Always apply with the screen fully extended. Make a second thin pass over all fold zones and edges. Allow full cure time before retracting — retracting before curing is complete will transfer wet coating to the housing and leave those panel sections uncovered.
Coating Effectiveness Diminishing Faster Than Expected
What you'll see: Microbiological indicators or facility HAI tracking suggests the coating is losing efficacy ahead of schedule.
Why it happens:
- High-frequency cleaning with alcohol-based wipes strips coatings faster than manufacturer estimates account for
- Physical abrasion compounds chemical wear: the 2024 ASEPTIC pilot trial — a randomized controlled study of a modified acrylate/silane coating on ED stretcher rails — found coating effect was lost where adhesive waste bags mechanically abraded the surface
Fix:
- Shorten reapplication intervals based on your facility's actual cleaning frequency
- Confirm with the manufacturer that your specific disinfection agents are compatible with the coating
- Consider coatings with documented alcohol solvent resistance if isopropyl alcohol wipes are standard in your protocol
Most of these problems are preventable with the right surface prep, application technique, and reapplication schedule — all of which your coating manufacturer should be able to specify for your exact partition material and cleaning protocol.
Pro Tips for Effective Antimicrobial Coating in Dialysis Environments
Schedule applications during planned shift downtime — not between patient sessions. Bay turnover pressure makes it nearly impossible to hit the full curing window reliably.
Non-porous surfaces cut long-term maintenance. Hospital-grade wipeable panels — like those on Rolascreen's Wall-Mounted Elite and Lite screens — hold coatings more durably and require fewer reapplication cycles than fabric-based alternatives.
Log every application without exception. At minimum, record the product name, lot number, application date, technician, and next reapplication date. This documentation protects you during accreditation audits and keeps reapplication intervals on track across all bays.
Frequently Asked Questions
What is an antimicrobial surface?
An antimicrobial surface is one engineered or treated to actively inhibit the growth and survival of microorganisms — bacteria, viruses, and fungi — on contact. This is distinct from a surface that is simply cleaned periodically; an antimicrobial surface provides continuous suppression of microbial activity between cleaning cycles.
What are antimicrobial coatings made of?
Common active chemistries include modified acrylates, silanes, quaternary ammonium compounds, silver nanoparticles, and copper-based materials. Selection depends on your surface type, target pathogens, and the disinfectants your facility already uses.
How long does antimicrobial coating last on dialysis bay partitions?
Longevity varies by product, but dialysis-specific conditions — high-frequency alcohol wipe-downs, mechanical contact, and patient proximity — typically shorten effective life well below manufacturer estimates. Facilities should establish reapplication schedules based on their own cleaning frequency, not general product labeling.
Do antimicrobial coatings replace regular cleaning in dialysis bays?
No. Coatings are a supplemental layer of protection that reduce microbial burden between cleaning cycles. Regular disinfection protocols must continue in parallel — EPA guidance classifies antimicrobial coatings as supplements to standard disinfection, not substitutes.
Can antimicrobial coatings be applied to retractable privacy screens?
Yes, provided the screen has non-porous panel surfaces, is fully extended during application, and fold and hinge zones are specifically addressed. Applying to a partially retracted screen leaves overlap areas untreated, which is one of the most common coverage failures in practice.
How often should antimicrobial coatings be reapplied in dialysis centers?
Standard manufacturer intervals — often measured in weeks or months — are typically derived from testing conditions that do not reflect dialysis-level cleaning frequency. Verify reapplication timing directly with the coating supplier, specifying your exact disinfection agents and the number of cleaning cycles per day your facility performs.