The problem isn't always cleaning frequency. It's what surfaces are made of.
This guide covers why specific surface materials create conditions where pathogens persist, what antimicrobial surface panels actually do, how to evaluate them for procurement, and what long-term management looks like in practice.
Key Takeaways
- MRSA, VRE, and C. diff survive on hospital surfaces for weeks to months — far outlasting standard cleaning intervals
- Porous, grouted, and fabric surfaces give pathogens physical shelter from disinfectants
- Bacterial contamination on bed rails rebounds to roughly 30% of pre-cleaning levels within 6.5 hours of disinfection
- Non-porous, seamless panels reduce microbial load between cleaning cycles
- Antimicrobial panels are one layer of defense; they don't replace hand hygiene, isolation protocols, or routine cleaning
Why Hospital Surfaces Become HAI Hotspots
HAIs don't arise from cleaning failures alone. They begin with surface materials that create conditions where pathogens can persist, hide, and transfer undetected. Understanding this distinction changes how facilities approach surface selection.
Pathogens Survive Far Longer Than Expected
Research published by Kramer et al. documents survival times that most clinicians find surprising:
| Pathogen | Survival Time on Dry Surfaces |
|---|---|
| MRSA | 7 days to 7 months |
| VRE | 5 days to 4 months |
| C. difficile spores | Up to 5 months |
| Norovirus | 8 hours to 7 days |
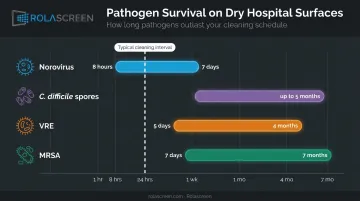
These figures reflect real-world hospital materials — plastics, fabrics, and stainless steel — under conditions similar to active patient areas.
The downstream risk is measurable. A cohort study of 1,770 medical ICU patients found that patients who moved into a room previously occupied by a CDI-positive patient had 11.0% CDI acquisition versus 4.6% in rooms with non-CDI prior occupants — a hazard ratio of 2.35. Those rooms received terminal cleaning.
Porous and Textured Surfaces Create Microbial Refuge
Surface micro-texture matters more than most facility managers realize. Studies show bacterial fouling can vary by up to 75-fold depending on surface roughness, nanostructure, and wetting properties. Pathogens don't just sit on surfaces; they find physical shelter in seams, grout lines, brushed-metal grooves, and fiber matrices.
Even stainless steel handrails with brushed finishes harbor microbes in their directional ridges. Mac Medical's IFU-041 specifically instructs users to scrub contaminated stainless surfaces with the grain to reduce this risk — a detail most EVS staff are never trained on.
That same design logic is codified in clinical guidelines. The AHE's health care furniture design guidelines specify that manufacturers should minimize surface joints and seams, since they create reservoirs for HAI-associated organisms. The FGI Guidelines go further, requiring floors and wall bases in operating rooms and isolation rooms to be monolithic, joint-free, or seamless.
High-Touch Surfaces and Cross-Contamination
Correct cleaning technique doesn't solve the recontamination problem. A study published in AJIC sampled bacteria on rails from 36 medical ICU beds before cleaning and at intervals up to 6.5 hours afterward. Hospital-approved disinfectants reduced bacterial burden by up to 99% immediately after cleaning, but contamination rebounded to approximately 30% of pre-disinfection levels by 6.5 hours.
High-touch surfaces — bed rails, equipment handles, door frames, and partition panels — get touched by dozens of hands between cleaning cycles. Without residual antimicrobial activity, recontamination begins immediately.
Fabric Privacy Curtains as Overlooked Vectors
Fabric curtains are among the most contaminated surfaces in patient care areas, yet they're among the least frequently cleaned. Research by Ohl et al. found that 92% of newly placed hospital curtains were contaminated within one week of installation, with pathogens including MRSA and VRE.
A separate survey found that curtains cleaned every four months had contamination rates of 42% VRE, 22% MRSA, and 4% C. difficile. Standard protocols in many facilities change curtains only every six months — or when visibly soiled.
Fabric simply cannot be wiped with hospital-grade disinfectants. Managing contamination requires full washing cycles or complete replacement — both of which leave significant gaps between interventions.
The Hidden Cost of Getting Surface Selection Wrong
The CDC estimates that on any given day, about 1 in 31 hospital patients has at least one healthcare-associated infection. AHRQ data puts the average additional inpatient cost per infectious HAC at approximately $31,000 — with CLABSI cases averaging $48,108 and C. difficile infections averaging $17,260.

These numbers assume a single case. HAI clusters tied to persistent surface contamination compound quickly.
Warning Signs Your Current Surface Materials Are Failing Infection Control
Three patterns should prompt a surface materials review:
Sign 1: Recurring HAI clusters in specific rooms or patient areas despite compliant cleaning protocols. When the pattern is location-specific rather than unit-wide, the surface is likely harboring pathogens between cleanings, not a technique problem.
Sign 2: Visible staining, discoloration, or degradation on panels or walls. This typically indicates disinfectant-material incompatibility. CDC guidance warns that chlorine-based disinfectants corrode metals above 1,000 ppm, and hydrogen peroxide can discolor anodized metal and damage certain polymers.
Damaged surfaces develop micro-texture that increases microbial attachment, compounding the contamination risk with every cleaning cycle.
Sign 3: Ongoing reliance on disposable curtain replacements or repeated re-cleaning in the same areas. If specific surfaces keep requiring re-cleaning or replacement, the material itself is the problem, not the cleaning frequency.
These warning signs tend to surface months after installation, once cleaning protocols and disinfectant chemistry begin interacting with the material at scale. At $31,000+ per HAC event, a single preventable cluster can dwarf the cost of specifying the right surface material upfront.
How Antimicrobial Surface Panels Work to Reduce Hospital Infections
Antimicrobial surface panels are one layer in a multi-modal HAI prevention strategy. They reduce microbial load between cleaning cycles — they don't eliminate the need for cleaning. That distinction matters when evaluating them.
Non-Porous Materials Block Microbial Attachment
The foundational requirement for any antimicrobial hospital panel is non-porosity. In clinical terms, this means a smooth, continuous surface with no seams, grout lines, or micro-textures that pathogens can colonize.
AHE guidelines specifically recommend nonporous smooth solid surfaces — such as laminate or poly resin — to support effective cleaning. Upholstered surfaces in patient care areas should be impervious and nonporous; the guidelines note that microorganisms can survive on porous fabrics including cotton, nylon, and polyester.
Non-porosity is a prerequisite. Antimicrobial properties — whether built-in or coated — provide limited benefit on a surface that already provides physical shelter for pathogens.
Integrated Antimicrobial Properties vs. Surface Coatings
Not all antimicrobial panels work the same way. The distinction between built-in and applied properties matters for long-term performance.
Material-integrated antimicrobial properties — copper alloy surfaces, silver-ion substrates — are part of the surface itself. Michels et al. found that copper alloy components in ICU clinical trials showed an 83% reduction in bacteria compared to standard surfaces, with HAI rates reduced by 58%.
Applied surface coatings offer convenience but carry durability limitations. A study evaluating silver-ion coatings documented performance at 24 hours, 7 days, 30 days, 60 days, and 180 days — with findings supporting caution about coating performance over time under real use conditions. A separate ED study of an antimicrobial surface coating found significant bacterial reduction initially, but the difference was not statistically significant at 180 days when coating integrity was compromised.
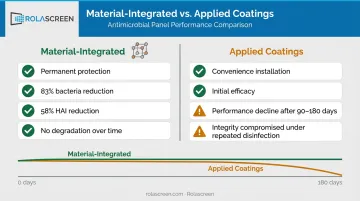
When specifying panels for long-term hospital use, ask manufacturers for performance data beyond 90 days under real cleaning protocols — not just initial lab results. That gap between early efficacy and sustained performance is where coating-based products most often fall short.
Replacing Fabric Privacy Curtains with Wipeable Panel Systems
Replacing fabric curtains with hard, wipeable privacy panels addresses the contamination gap directly. Instead of managing a curtain-exchange logistics cycle, surface disinfection becomes part of a routine wipe-down.
Rolascreen's retractable privacy screen panels, manufactured in Chatsworth, California, use non-porous thermally-stabilized polyester film. The inner panel surface has no fiber matrix or wicking properties, so pathogens cannot penetrate or shelter within the material. Panels are validated for sodium hypochlorite up to 10,000 ppm (above the CDC's 5,000 ppm sporicidal threshold for C. diff), quaternary ammonium compounds, accelerated hydrogen peroxide at 4.5%, and alcohol-based wipes.
Cleaning requires no disassembly. A staff member wipes top-to-bottom with a standard disinfectant wipe — completing the full panel in approximately two minutes. No curtain exchange. No laundry cycle. No gap in coverage while the area waits for reinstallation.
Compatibility with Hospital-Grade Disinfectants
Antimicrobial surface panels must be tested against the disinfectant categories actually used in the facility. Incompatible materials degrade under repeated disinfection; surface degradation increases microbial attachment risk and voids efficacy claims.
The major disinfectant categories used in US hospitals include:
- Quaternary ammonium compounds (CaviCide, Virex)
- Sodium hypochlorite / bleach-based solutions
- Accelerated hydrogen peroxide (Virox, Oxivir)
- Alcohol-based products (60–80%)
Require documented compatibility testing for all categories before procurement. If a manufacturer cannot provide it, treat that as a disqualifying gap — not a documentation oversight.
What to Look for When Selecting Antimicrobial Surface Panels
Surface Material and Porosity Standards
Specify panels with smooth, non-porous, minimal-seam surfaces. Materials that meet this standard include:
- Solid-core composites
- PVC
- High-pressure laminate (HPL)
- Non-porous polyester film
Avoid grouted tiles, plasterboard finishes, woven textiles, or any material with exposed seams in patient care zones. For mobile or retractable partition panels, surface standards should match fixed wall panels — non-absorbent, ridge-free, and wipe-compatible.
Once you've confirmed surface material, verify it holds up to the disinfectants your EVS team already uses.
Disinfectant Compatibility Documentation
Request documented compatibility testing for at least bleach-based and quaternary ammonium products before purchase. These are the two most commonly used categories in US hospital environments.
Absence of multi-disinfectant testing creates a real risk: applying the wrong disinfectant damages the surface, creating micro-texture that increases contamination and voids the panel's efficacy claims.
Material and disinfectant compatibility only matter if the surface holds up over months of daily use. Durability under real hospital conditions is the third checkpoint.
Durability Under Hospital Conditions
Evaluate panels for:
- Repeated chemical wipe-down without surface degradation (peeling, pitting, discoloration)
- Physical contact from equipment and staff without structural compromise
- For portable systems: flexing, transport, and repositioning without surface integrity loss
For portable and retractable systems, US-manufactured products offer a practical advantage — faster quality control resolution, domestic warranty support, and clearer accountability when surface performance issues arise. Rolascreen's interchangeable zippered panel design, for example, lets individual panels be swapped without replacing the entire frame — reducing both the cost and the delay of addressing a degraded surface.
Ease of Cleaning and Staff Adoption
Even a clinically superior surface fails if staff can't clean it quickly and consistently. The simpler the process, the higher the compliance during busy shifts.
Look for panels that require no specialized cleaning agents, no directional wiping technique, and no disassembly before cleaning. Surfaces that fit naturally into existing EVS workflows see measurably higher compliance — particularly during high-volume shifts when shortcuts are most tempting.
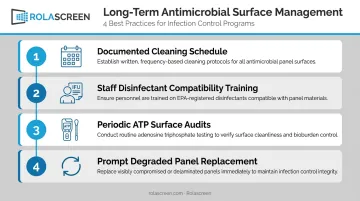
Best Practices for Long-Term Antimicrobial Surface Management
Antimicrobial panels reduce microbial load between cleanings. They don't eliminate the need for disciplined hygiene programs. Long-term control requires both the right materials and the right practices.
- Establish a documented cleaning schedule for all panel surfaces, including mobile privacy screens and room dividers, with assigned responsibilities by role and shift
- **Train staff on disinfectant compatibility** for specific panel types using manufacturer IFUs; document that training as part of infection control compliance records
- Conduct periodic surface audits with ATP bioluminescence testing, which the CDC includes among environmental cleaning monitoring methods for rapid contamination feedback
- Replace degraded panels promptly: cracking, pitting, staining, or delamination means antimicrobial effectiveness is gone — remove the panel from clinical use
Note: ATP testing detects organic residue, not specific pathogens. It's a contamination indicator, not a pathogen screen.
Pairing the right surface materials with consistent staff protocols gives infection control programs the greatest long-term return on any panel investment.
Frequently Asked Questions
What do hospitals use to disinfect surfaces?
Hospitals use EPA-registered disinfectants including quaternary ammonium compounds, bleach-based solutions, hydrogen peroxide products, and alcohol-based agents. The disinfectant selected must be compatible with the specific surface material being cleaned — incompatible combinations damage surfaces and reduce effectiveness over time.
What makes a surface panel truly antimicrobial in a hospital setting?
An effective antimicrobial hospital panel must be non-porous to block microbial attachment, incorporate durable or built-in antimicrobial properties, and be verified as compatible with the hospital's standard disinfectants. All three criteria must be met — no single property is sufficient on its own.
Are privacy screens and room divider panels a source of hospital-acquired infections?
Fabric-based privacy curtains are documented HAI vectors — 92% become contaminated within one week of installation, and they cannot be wiped with hospital-grade disinfectants. Replacing them with non-porous, wipeable hard-surface panel systems significantly reduces this risk.
How often should antimicrobial surface panels be cleaned in a hospital?
Cleaning frequency should follow the same protocol as other high-touch surfaces in that care area — typically between each patient use in acute and ED settings, with disinfectant selection guided by the manufacturer's Instructions for Use (IFUs).
What is the difference between antimicrobial surface panels and standard hospital panels?
Standard panels focus on durability and cleanability. Antimicrobial panels add an active layer of protection — through built-in materials like copper or silver-ion technology, or through durable compatible coatings — that reduces bacterial load between cleaning cycles.
Can antimicrobial surface panels replace other infection control measures?
No. Antimicrobial panels reduce surface microbial burden between cleanings but do not replace hand hygiene, proper PPE use, isolation protocols, or routine disinfection by staff. They work alongside these measures — not instead of them.