Research documented in SHEA's isolation precautions guidance links visitors to healthcare-associated outbreaks of TB, SARS, H1N1 influenza, norovirus, and MERS-CoV — with at least 21 SARS cases in Singapore and a pediatric TB outbreak involving 24 children traced to visitor transmission. Compliance data makes the picture worse: only about 10% of visitors perform hand hygiene when entering or leaving a patient room.
This guide is written for healthcare facility administrators, infection control staff, and visitors themselves. It covers what standard precautions apply to everyone entering a patient care area, how requirements escalate based on the type of infection present, and what facilities can do to close the compliance gap.
Key Takeaways
- Hand hygiene — sanitizer or soap and water — is non-negotiable on entry to and exit from every patient room, not just the ward entrance.
- Stay home if you've had diarrhea, vomiting, fever, rash, or an uncontrolled cough within the last three days.
- Contact, droplet, and airborne precautions each require different visitor behaviors — follow the posted signs on every patient room door.
- High-risk units (oncology, ICU, transplant, NICU) apply stricter visitor screening than general wards — always confirm before arriving.
- Ask staff about precaution requirements at entry — facilities vary widely in how clearly they communicate them.
Why Visitor Infection Control Is Critical in Healthcare Settings
Hospitals concentrate people who cannot afford an infection: post-surgical patients, immunocompromised individuals receiving chemotherapy, transplant recipients on immunosuppressants, and premature infants in NICUs. A pathogen that causes three days of inconvenience in a healthy adult can be life-threatening in any of these populations.
The scale of what's at stake is documented. According to the CDC, the HAI burden in U.S. hospitals is substantial:
- On any given day, approximately 1 in 31 hospital patients has at least one HAI
- In 2015, an estimated 687,000 HAIs occurred in U.S. acute care hospitals
- Those infections contributed to roughly 72,000 deaths during those hospitalizations
- Direct medical costs run between $28.4 billion and $45 billion annually

Visitors are not peripheral to this problem. The CDC and SHEA both structure infection control in two tiers:
- Standard Precautions — applied universally to all patient care interactions, regardless of diagnosis
- Transmission-Based Precautions — layered on top for specific pathogens requiring additional controls
Both tiers apply to visitors, not just clinical staff. SHEA's visitor-specific guidance explicitly requires hand hygiene for all visitors and pathogen-appropriate contact, droplet, or airborne practices when indicated. Most visitors are never informed of these expectations, and most facilities don't have a consistent system for communicating them.
Before You Visit: Health Screening and Preparation
Self-Screening Before You Leave Home
APIC guidance states clearly: do not visit a healthcare facility if you have experienced nausea, vomiting, diarrhea, fever, an uncontrolled cough, or a rash within the last three days. That three-day window reflects how long common pathogens typically remain transmissible.
Beyond GI and respiratory symptoms, check whether you've had recent exposure to:
- Chickenpox or shingles — requires airborne plus contact precautions; susceptible visitors should not enter affected rooms
- Measles — CDC restricts visitors without acceptable evidence of immunity from entering rooms with known or suspected measles
- Mumps — droplet precautions apply for five days after onset of parotid swelling
If you're unsure whether your recent exposure disqualifies you, call the ward before arriving. Ward staff can quickly confirm whether your visit is safe to proceed.
High-Risk Units Require Extra Steps
General wards have baseline visitor requirements. High-risk units apply stricter criteria, and the CDC recommends targeted screening for visitors to:
- Oncology and hematology units
- Hematopoietic stem cell transplant (HSCT) units
- ICUs and severely immunocompromised patient areas
- Neonatal intensive care units (NICUs)
For HSCT units specifically, CDC guidance recommends that visitors with any upper respiratory or flu-like symptoms defer their visit entirely until symptoms resolve.
These rules apply to general visitors. Extended-stay caregivers — parents, guardians, and primary caregivers who lived with the patient before hospitalization — are treated differently.
A Note on Extended-Stay Caregivers
SHEA acknowledges that extensive prior household exposure may mean these individuals are already immune or past the incubation window. Facilities may apply modified or less restrictive precautions in these cases, but that determination belongs to the ward team, not the visitor.
Standard Infection Control Precautions for All Hospital Visitors
These apply regardless of why the patient is admitted and regardless of whether any isolation sign is posted.
Hand Hygiene
The two-method approach:
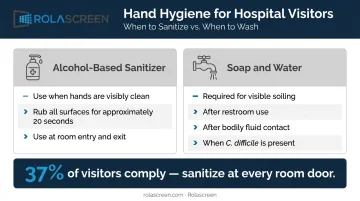
- Alcohol-based hand sanitizer — use when hands are visibly clean; rub over all surfaces until dry (approximately 20 seconds)
- Soap and water — required when hands are visibly soiled, after using the restroom, after any contact with bodily fluids, and whenever C. difficile is present on the ward (soap and water is preferred because alcohol-based products are less effective against spore-forming organisms)
Hand hygiene must occur on entry to and exit from every patient room — not just at the ward entrance. This distinction matters more than almost anything else in this guide. A 2025 meta-analysis found pooled visitor hand hygiene compliance of just 37% across 17 observational studies. SHEA puts compliance at room entry and exit closer to 10%.
Respiratory Etiquette
- Cover coughs and sneezes with a tissue or your elbow — not your hand
- Dispose of used tissues immediately
- Perform hand hygiene after
If you have respiratory symptoms, don't visit — reschedule until symptoms resolve. Even asymptomatic visitors should follow respiratory etiquette as a default.
Behavioral Controls
These rules reduce indirect transmission through contaminated surfaces:
- Do not sit or lie on the patient's bed
- Do not touch medical equipment, dressings, IV lines, or drainage devices
- Use visitor chairs, not patient furniture
- Supervise children to prevent floor contact and surface touching
Limiting Contamination Pathways
- Bring only essential personal items into patient areas
- Store bags and belongings away from bed surfaces and equipment
- Do not enter ward kitchens unless explicitly permitted
- Check whether flowers or outside food are allowed — some wards restrict both
Physical Environment and Spatial Separation
Open-bay wards carry higher cross-contamination risk than single-room settings. A 2024 meta-analysis of 12 studies and 12,718 patients found that single-patient rooms were associated with lower nosocomial infection odds (OR 0.68) and lower multidrug-resistant organism acquisition odds (OR 0.41) compared to multi-patient rooms.
Where single rooms aren't available, physical separation still reduces risk. CDC guidance calls for:
- At least 3 feet of spatial separation between beds for droplet-route infections
- Curtain or screen use to delineate patient zones
- Barriers that can be reliably disinfected between patient contacts
Retractable privacy screens — used at UCSF, Kaiser Permanente, and VA facilities — address the last point directly. Fabric curtains can't be included in terminal cleaning protocols; screens with non-porous, wipe-clean film panels (compatible with bleach, quats, and accelerated hydrogen peroxide) can be. Rolascreen supplies these to over 900 healthcare facilities across the US.
Physical barriers reinforce the precautions in this guide — they don't replace them. Hand hygiene, respiratory etiquette, and visitor screening remain the first line of defense.
Transmission-Based Precautions: Visitor Responsibilities by Infection Type
A sign posted on a patient room door or bay curtain tells you what precaution tier is active. Read it before entering. If the sign is unclear, ask a nurse before going in.
Contact Precautions for Visitors
Contact precautions cover pathogens spread through direct or indirect physical touch. SHEA's position: routine contact precautions for visitors are not recommended for endemic MRSA or VRE, but are appropriate for C. difficile, norovirus, and extensively drug-resistant gram-negative organisms (KPC/CRE).
Visitor responsibilities:
- Perform hand hygiene before entering and immediately after leaving
- Do not touch bed linens, dressings, or any patient care equipment
- Do not visit other patients after leaving a contact-precaution room
- Wear gloves and gown if assisting with any aspect of care
Droplet Precautions for Visitors
Droplet precautions apply when a pathogen spreads through large respiratory droplets — coughing, sneezing, or talking. Common examples include influenza, pertussis, and bacterial meningitis.
Visitor responsibilities:
- Put on a surgical mask before entering and keep it on throughout the visit
- Perform hand hygiene on entry and exit
- Follow any additional eye protection guidance from nursing staff
- Siblings of pediatric patients are generally discouraged from shared spaces such as playrooms
Airborne Precautions for Visitors
Airborne precautions apply to pathogens that travel as small suspended particles over long distances — tuberculosis, measles, and varicella (chickenpox). These rooms use negative-pressure airflow to contain particles.
Visitor responsibilities:
- Verify immunity or vaccination status before entering — confirm varicella immunity, for instance, before visiting a chickenpox patient
- Wear an N95 respirator; proper N95 use requires fit testing, and a surgical mask is a less effective alternative when fit testing isn't available
- Keep the room door closed at all times
- Consider whether the visit is medically necessary given the level of protection required
- Facilities may limit visitation for visitors who cannot document immunity to the pathogen in question, per SHEA guidance

Common Infection Control Mistakes Visitors Make
Skipping Hand Hygiene at the Room Door
The dispenser at the ward entrance feels like the main checkpoint. It isn't. Hand hygiene must happen at the patient room door — both entering and leaving. Colonized organisms on hands are invisible; the absence of perceived exposure doesn't mean the absence of transmission risk.
Visiting While Symptomatic
Visitors consistently underestimate mild symptoms. A low-grade cough or one episode of loose stool seems trivial. For a patient on immunosuppressive therapy, it isn't.
The standard threshold exists because pathogens remain transmissible before symptoms fully resolve — and after they seem to improve. Stay home if you have any of the following within the past three days:
- Fever
- GI symptoms (vomiting or loose stool)
- New rash
- Uncontrolled cough
The 2009 H1N1 outbreak on a pediatric hematology-oncology ward, in which a hospital visitor was identified as the source of six cases, is a documented example of what "mild" visitor illness can produce in a vulnerable inpatient population.
Treating Isolation Signs as Optional
Isolation signage is not informational. It's instructional. Visitors who ignore a contact or droplet precaution sign — or who assume that gowns and masks are only for staff — don't just affect the patient in the room. They become vectors who may carry the pathogen to other patients, to staff, and back into the community.
SHEA data puts MRSA contact-precaution adherence among visitors at 11% and gown adherence between 49% and 65%. If you're unsure whether a precaution applies to you, ask the nurse at the station before entering. That question takes 30 seconds.
Frequently Asked Questions
What are the three types of transmission-based precautions that affect hospital visitors?
Contact, droplet, and airborne precautions correspond to different pathogen transmission routes. Each requires different PPE and behavioral measures for visitors — contact and droplet may require masks or gowns, airborne requires an N95. Requirements are communicated via signage at the patient's room or bay curtain.
Do hospital visitors have to wear gloves and gowns when visiting a patient in isolation?
It depends on the precaution type and whether the visitor is assisting with care. Contact precautions may require gloves and gowns; droplet precautions typically require a surgical mask. Always confirm specific requirements with the nursing team rather than assuming PPE is optional.
When should a visitor stay home rather than going to the hospital?
Stay home if you've had diarrhea, vomiting, fever, rash, or an uncontrolled cough within the last three days. Also defer your visit if you've had recent exposure to a communicable condition like chickenpox or measles without first confirming your immunity status with ward staff.
Can children visit patients who are under contact or droplet precautions?
Children are generally discouraged from visiting patients under active transmission-based precautions. Siblings of pediatric patients on droplet precautions are typically restricted from communal areas. The ward team makes the final call based on the specific pathogen and the child's age and health status.
How is visitor hand hygiene different from what healthcare workers are expected to do?
The underlying technique is the same — alcohol gel for visibly clean hands, soap and water for visible soiling. Healthcare workers follow the WHO's "5 Moments for Hand Hygiene" during specific care tasks. Visitors follow a simplified version: clean hands before entering and after leaving every patient room.
What can healthcare facilities do to improve visitor compliance with infection control precautions?
Three practical strategies work well: post clear signage with accessible PPE supplies at room entry points (not just ward entrances); give first-time visitors to isolation patients a brief verbal briefing from nursing staff; and use physical barriers such as retractable privacy screens to delineate patient zones in open-bay settings and reduce incidental cross-contact.